

Overview
Galderma operates at the precise intersection of medical science and aesthetic artistry. For years, their reputation was built on a “mouth-to-mouth” training model—an internal term for face-to-face knowledge transfer where experts orally taught facial assessment (AART) and treatment (HIT). While effective for the elite few, by 2021, this manual system was straining under global demand and escalating operational costs. With 100,000+ healthcare professionals (HCPs) across 40+ markets needing training, the “mouth-to-mouth” model failed to sustain engagement; users would attend a workshop and then churn, lacking a mechanism to form a clinical habit. The ecosystem was disconnected, with many practitioners remaining in a “Dormant” or “Non-Activated” state. We weren’t just solving a content distribution problem; we were solving a user retention and activation problem. I improved the high-touch AART & HIT methodologies from exclusive in-person workshops into a scalable Product-Led Growth ecosystem. By mapping clinical education to a strict “Activation → Aha! → Habit” framework, we empowered 100,000+ practitioners to master facial assessment, digitizing the art of injection to drive premium portfolio adoption and reduce training variance.
Research & Design
Core Disciplines: Product-Led Growth (PLG) Strategy · Design-Led Research · Platform Design · Engagement State Modeling · Medical Education Regulatory Compliance · Interactive Assessment Tools · UX & UI Design · Digital Learning Pathways · Business model design
- Duration: June - December 2021
- Partners: Galderma Medical Education Team (Miriam Garcia), Global Digital Aesthetics (Pierre Geiger), Brand Strategy (Jennifer Younes), Digital HCP Content (Sara Olofsson), IT Business Analysis (Anne-Laure Donzé)
- Team: Thought Cab Design (Fas Lebbie, Daniel Borer, Sabrina Fessler) & Galderma Internal Design (David Sohrabian)
Confidentiality: The insights and design process shared in this case study reflect my perspective and design approach while respecting Galderma's confidentiality.
My Role
I introduced the User Engagement State framework to Galderma, moving stakeholders from a "content library" mindset to a "growth funnel" mindset. I defined the critical thresholds for Setup, Aha!, and Habit moments, aligning the design roadmap to optimize for "Activation" rather than just "Registration
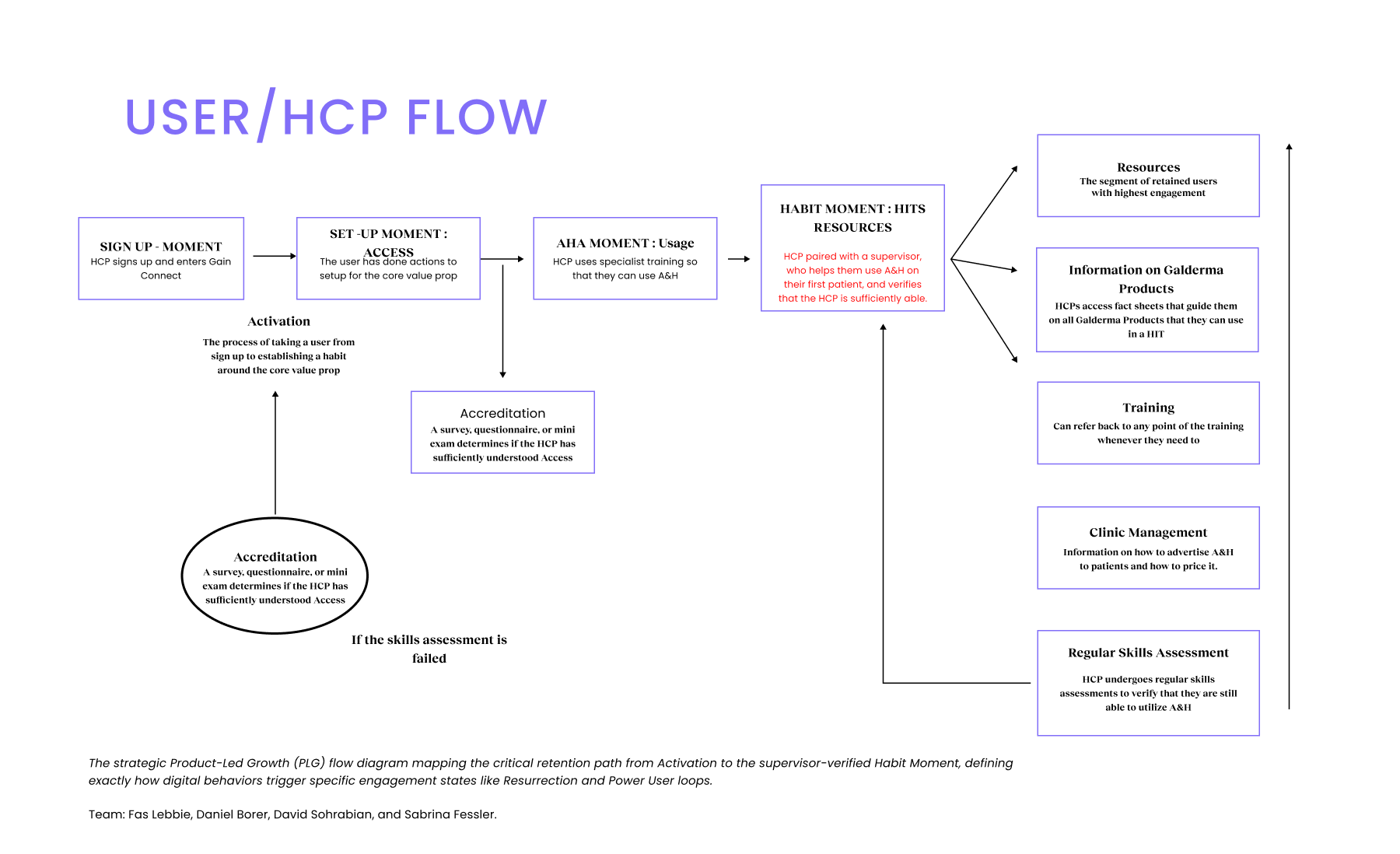
I led the ethnographic inquiry into the "mouth-to-mouth" system to identify what constituted a true "Aha! Moment" for a doctor. I synthesized these findings to define the "Habit Moment" as the specific point where an HCP is paired with a supervisor for their first patient interaction, shifting the focus from "content consumption" to "verified capability"
I architected the HCP Flow to function as a retention engine. This involved designing "Resurrection" loops in which failed accreditation assessments automatically triggered reactivation flows, and structuring "Power" user features such as Clinic Management and Resources to drive long-term engagement loops.
I navigated the friction between Brand Strategy (Jennifer Younes) and Digital Aesthetics (Pierre Geiger) by using the PLG framework as a neutral source of truth. By defining "Activated" and "Power" states, I aligned distinct business units on shared KPIs, helping the team prioritize an "Innovation Viable Product" (IVP) for the Brazil pilot that specifically tested the Time-to-Aha.
Problem Context
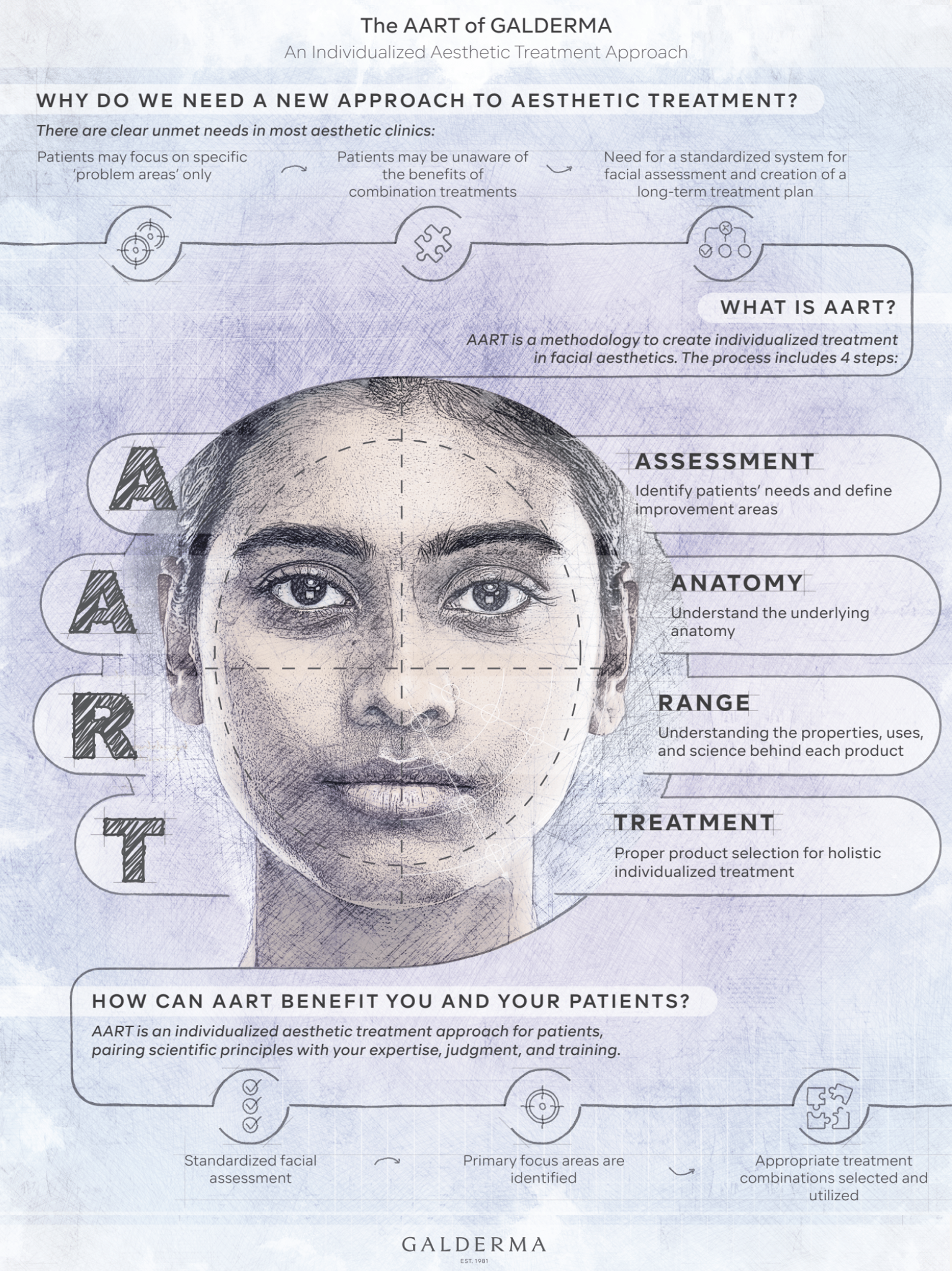
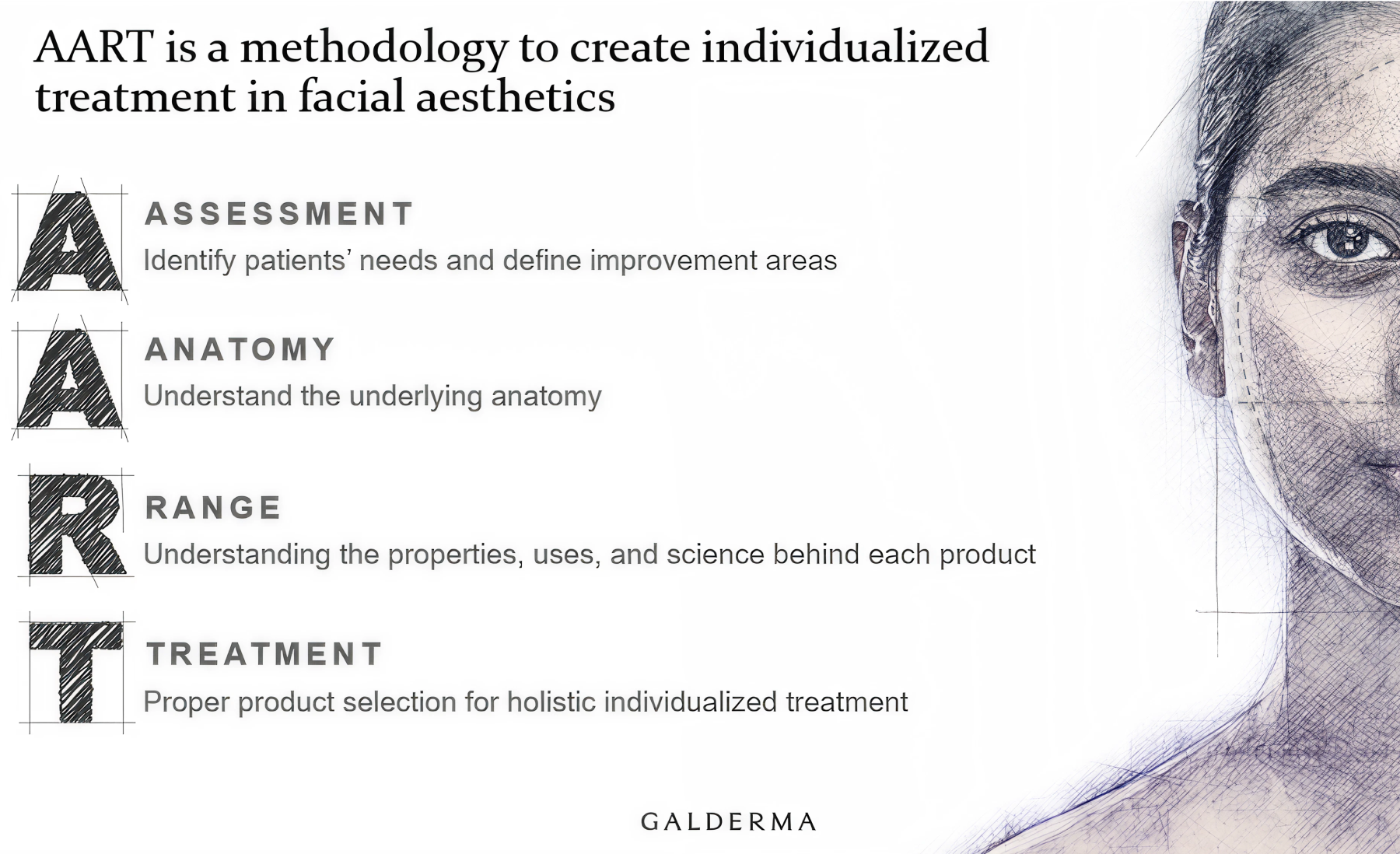
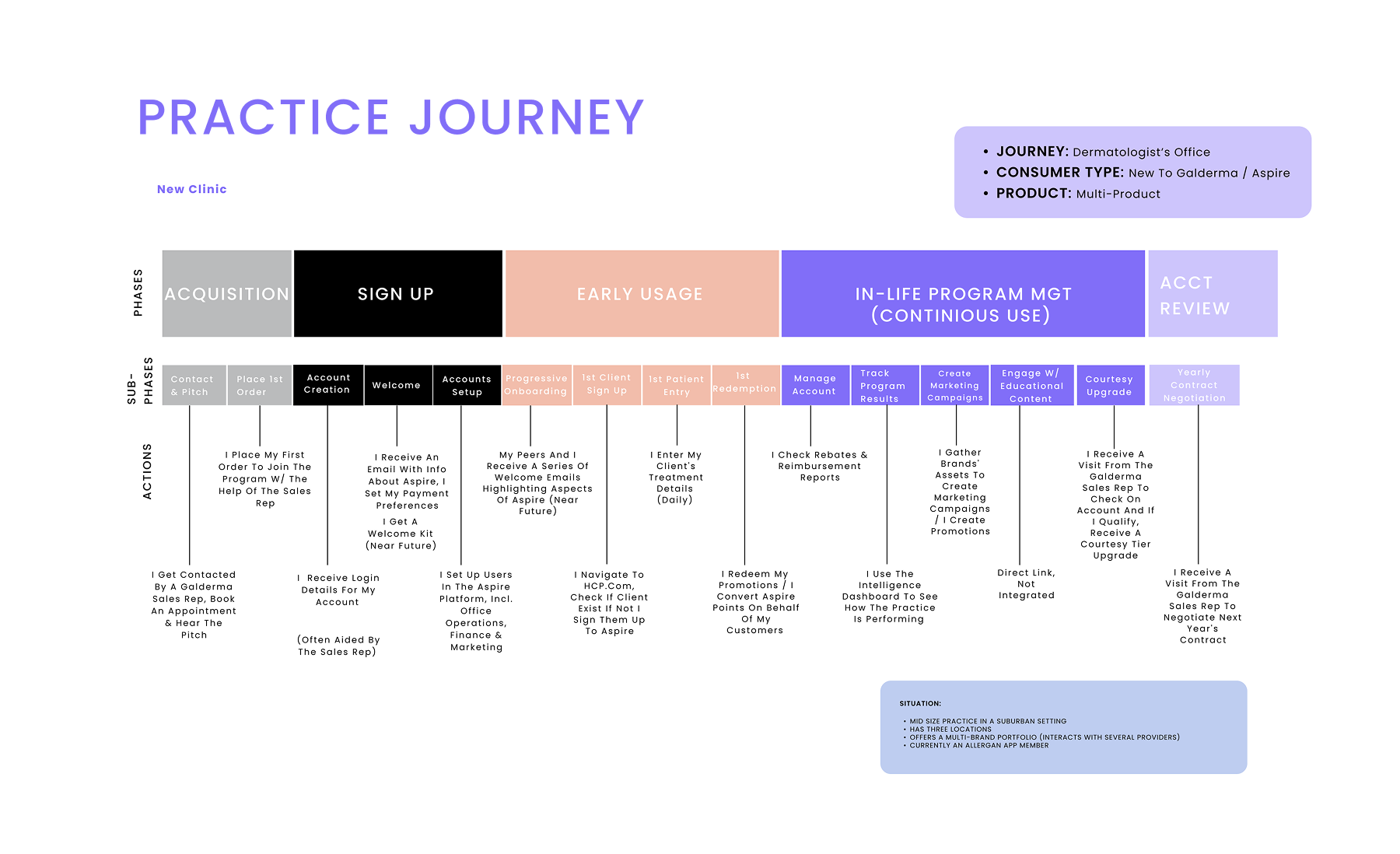
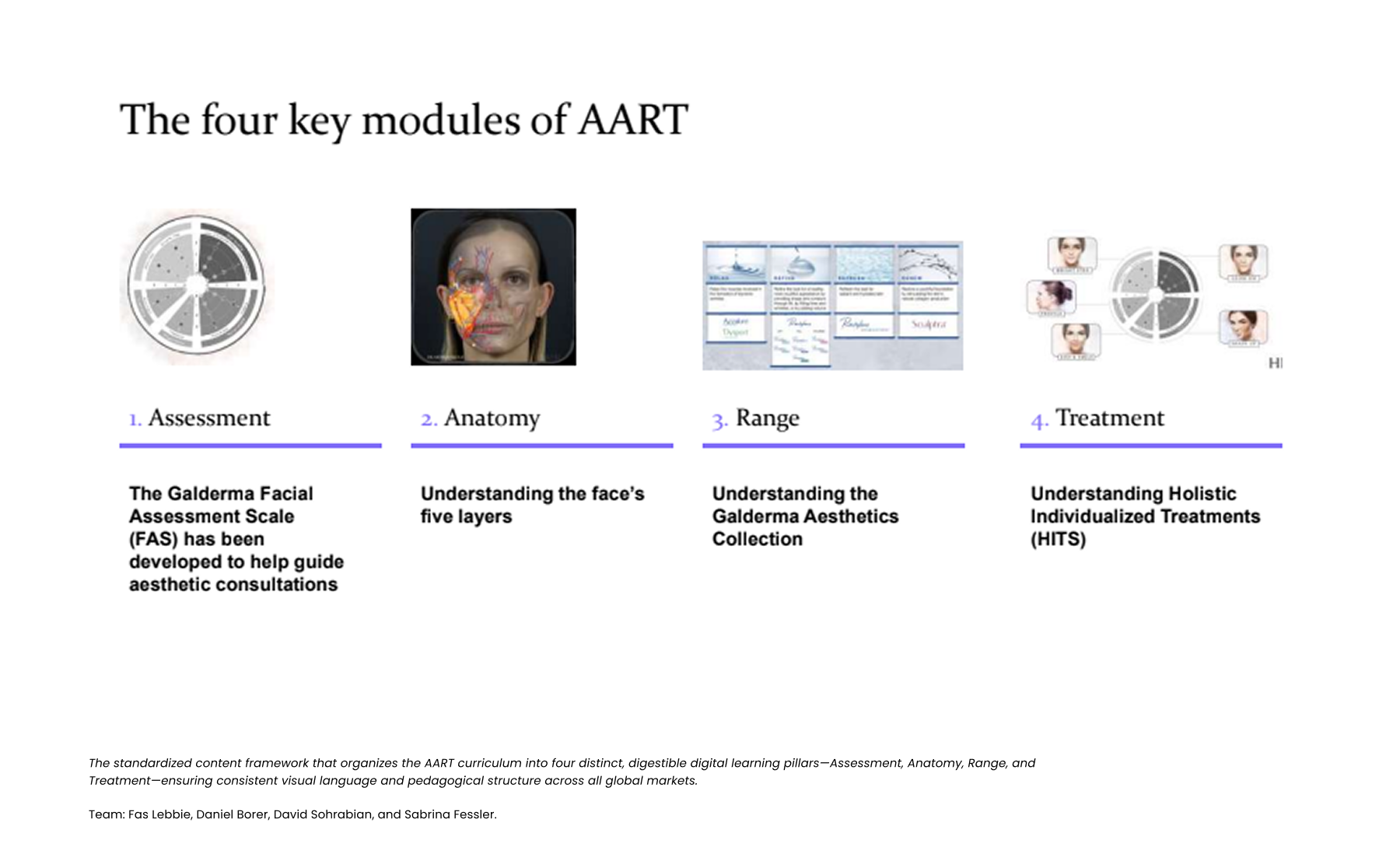
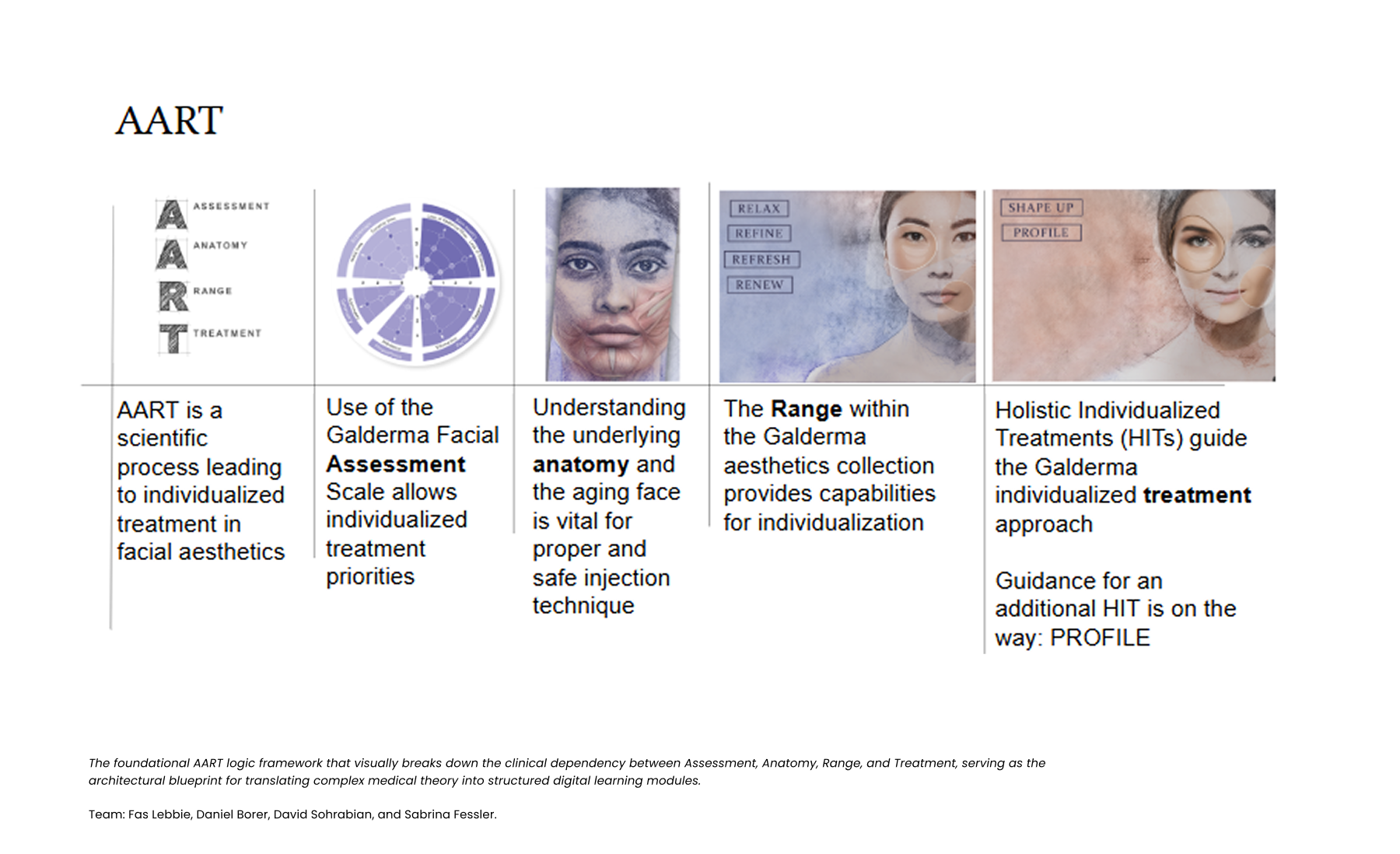
The central tension at Galderma was a disconnect between the sophistication of their methodology and the stickiness of their training. The AART (Assessment) and HIT (Treatment) systems represent a paradigm shift in aesthetics. However, teaching this through a “mouth-to-mouth” system created a leaky funnel: users would “Sign Up” physically but never reach the “Habit Moment” digitally. In the data, we saw a massive population of “Non-Activated” users. While practitioners utilized products, they did so without the “Setup Moment” required to access the core value prop. Without an expert standing over their shoulder to enforce the habit, injectors churned back to old methods, unable to recall complex HIT protocols.
Organizational friction compounded this. The “solution” had been batch communication (slides), which offered no “Resurrection” path for users who dropped off. The business risk was clear without reaching the “Habit Moment,” practitioners wouldn’t adopt the premium portfolio. We needed a design intervention that functioned as a growth engine to bridge the gap between “Signed Up” and “Habit Established.”
My Approach
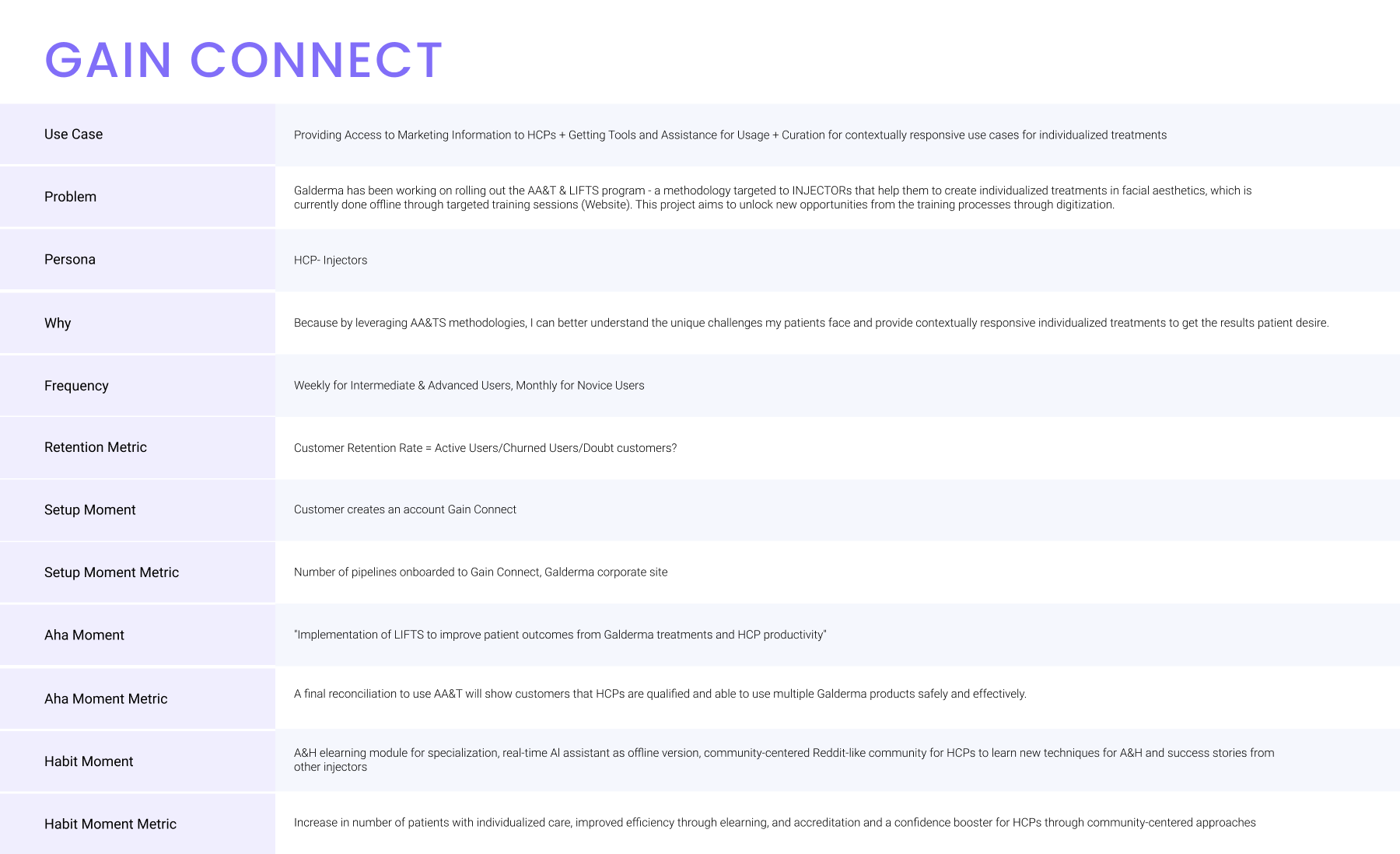
My philosophy was to treat medical competency as a Product-Led Growth funnel. I adapted standard PLG frameworks to the clinical environment, defining the “Aha! Moment” not as “finishing a video,” but as “using specialist training to unlock AART”. My execution focused on engineering the Setup Moment (Access) to reduce friction, ensuring users reached the Habit Moment (treating a patient) before they could churn.
Design Process
When we arrived, the “digital” landscape at Galderma was largely a repository of disconnected assets. The gold standard tool, the AART assessment disk, was a physical, analog object used in workshops. It was brilliant but unscalable and impossible to track usage data on.
We started with a wealth of medical content but a poverty of user experience. The “mouth-to-mouth” system meant knowledge was siloed with specific SMEs. Early observations showed that while the material was clinically accurate, the delivery was fragmented; Brazil, the US, and Australia each operated their own versions of GAIN Connect with little consistency.
The baseline data was sobering: engagement with existing e-learning materials was passive, largely consisting of “interactive videos” with limited capability. We found that 78% of practitioners struggled to translate theoretical knowledge from these static formats into consistent practice. Essentially, the starting line was a leaky bucket with zero visibility into learner drop-off points.
We knew we couldn’t just “guess” at how to build habits. We adopted a robust Discovery phase to define the specific clinical actions that constituted PLG states.
Methods & Participants We engaged directly with the “Medical Education Team” to map the “mouth-to-mouth” journey to the PLG framework. We conducted 1:1 semi-structured interviews with key stakeholders, including Jennifer Younes (Brand) and Miriam Garcia (Medical Education), to define what constituted a true “Aha! Moment”.
Early Insights & PLG Definition
- Defining “Aha!”: We identified that the “Aha Moment” wasn’t watching a video; it was “Using specialist training to use A&H”. This shifted our design to prioritize interactive tool usage immediately after setup.
- Defining “Habit”: We learned that clinical confidence requires verification. We defined the “Habit Moment” as “HCP paired with a supervisor who verifies they are sufficiently able”.
- Defining “Resurrection”: We realized failure was an opportunity. We designed the “Hail Mary Resurrection” path for users who failed assessments, routing them back to specific training modules rather than letting them churn.
Our investigation revealed that adoption barriers were structural, not intellectual. The original “mouth-to-mouth” model lacked the behavioral triggers necessary for habit formation.
- Insight: Content without context creates churn. Meaning: Users could access advanced HIT protocols without understanding the foundational AART assessment, leading to confusion and exit. Implication for Design: We instituted a Dependency Flow where HIT content is locked until AART mastery is demonstrated. This “gated” progression forces the user through the “Setup” and “Aha!” states in the correct order .
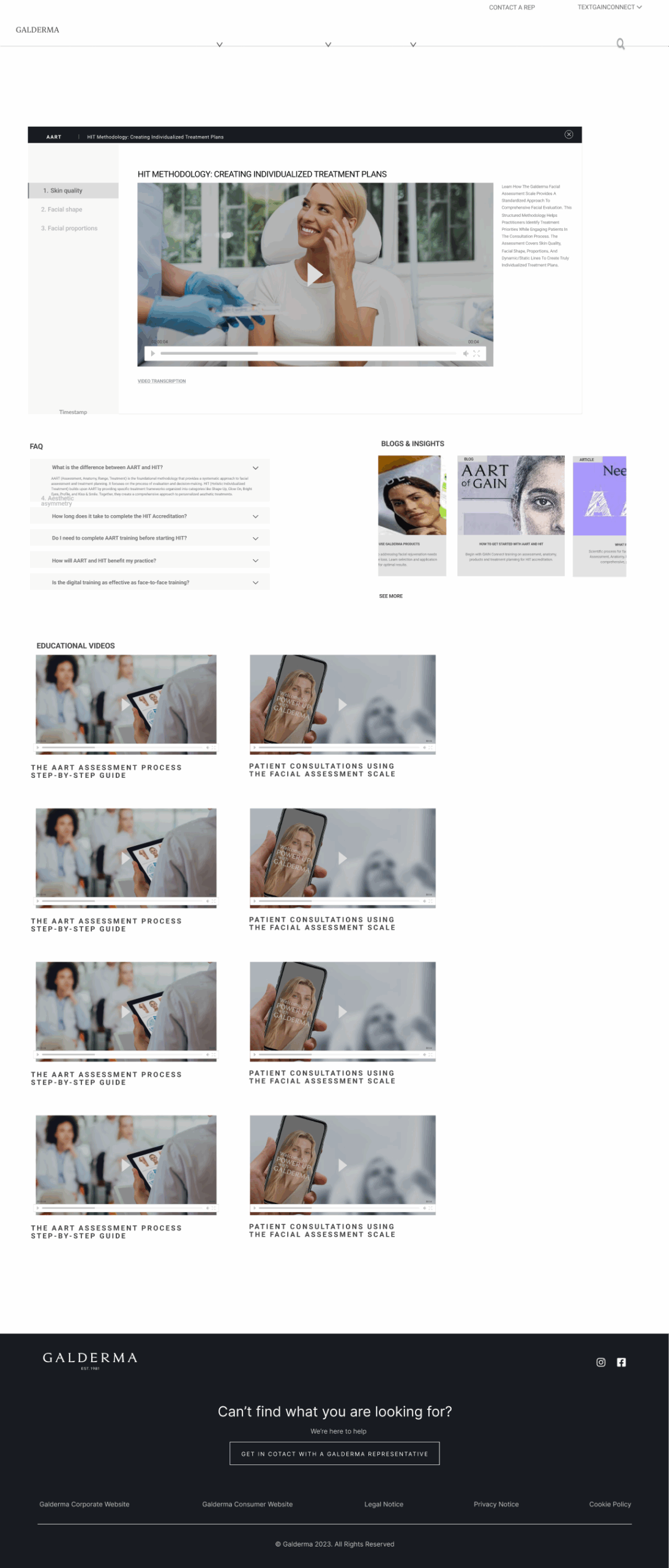
- Insight: Clinical confidence requires visual validation. Meaning: Text-based learning failed to build the “muscle memory” needed for facial assessment. Implication for Design: We developed the Interactive Facial Assessment Scale (FAS) as the core “Aha!” feature. Users must visually identify patient characteristics, turning passive learning into active diagnosis.
- Insight: Assessment failure is a high-churn moment. Meaning: When users failed a quiz, they often abandoned the platform entirely. Implication for Design: We built “Smart Resurrection” Loops. Instead of a generic “Fail” screen, the system redirects users to specific micro-lessons (e.g., “Review Facial Layers”) related to their errors, keeping them in the engagement funnel.
To ensure the platform delivered clinical value, we defined strategic goals that mapped directly to the User Engagement States visualized in our PLG framework.To ensure the platform delivered clinical value, we defined strategic goals that mapped directly to the User Engagement States visualized in our PLG framework.
- Goal: Activation Velocity (Setup to Aha!) The Challenge: Users were stuck in “Non-Activated” states, registering but never engaging the core AART value. The Goal: We aimed to reduce Time-to-Aha by streamlining “Access” actions. We measured success by the percentage of users unlocking the interactive assessment tool within their first session, moving swiftly from “Signed Up” to “Aha Moment”.
- Goal: Habit Formation (Aha! to Habit) The Challenge: Users would consume content (“Casual” state) but fail to apply it in clinic (“Core” state). The Goal: We targeted the Habit Moment Conversion Rate, specifically measuring the transition from digital training to the supervisor-verified “first patient” interaction.
- Goal: Resurrection & Retention The Challenge: High churn rates after initial workshops with no path back for “Dormant” users. The Goal: We sought to drive Resurrection via Accreditation Loops, ensuring that a failed skills assessment triggered a specific re-training flow rather than exit.
We worked backward from the “Habit Moment.” The prototyping phase was intense and iterative, driven by the need to navigate the strict regulatory landscape of the Brazil pilot market.
Fidelity & Iteration We utilized a “Skateboard / Scooter / Car” model to manage scope. The “Skateboard” MVP focused solely on Activation Flow testing to determine whether users could complete the “Setup Moment” (Access) and reach the “Aha Moment” (Usage). We stripped away non-essential “Casual” features to focus on this core conversion loop.
Collaboration & Validation We briefed the Build Team using the User Engagement State diagram as the architecture map. We validated the “Access” actions with 15 HCPs in Brazil, ensuring the “Setup Moment” wasn’t overly burdensome and effectively bridging the gap between creative vision and the friction of clinical reality.
Design Interventions
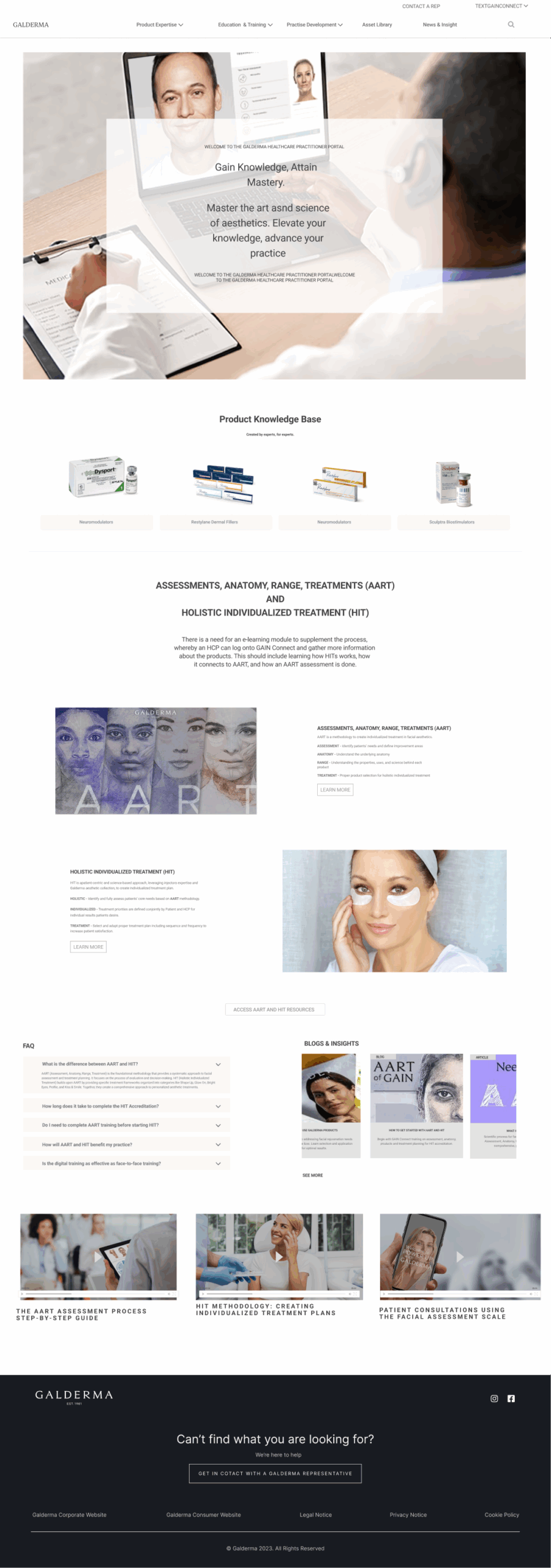
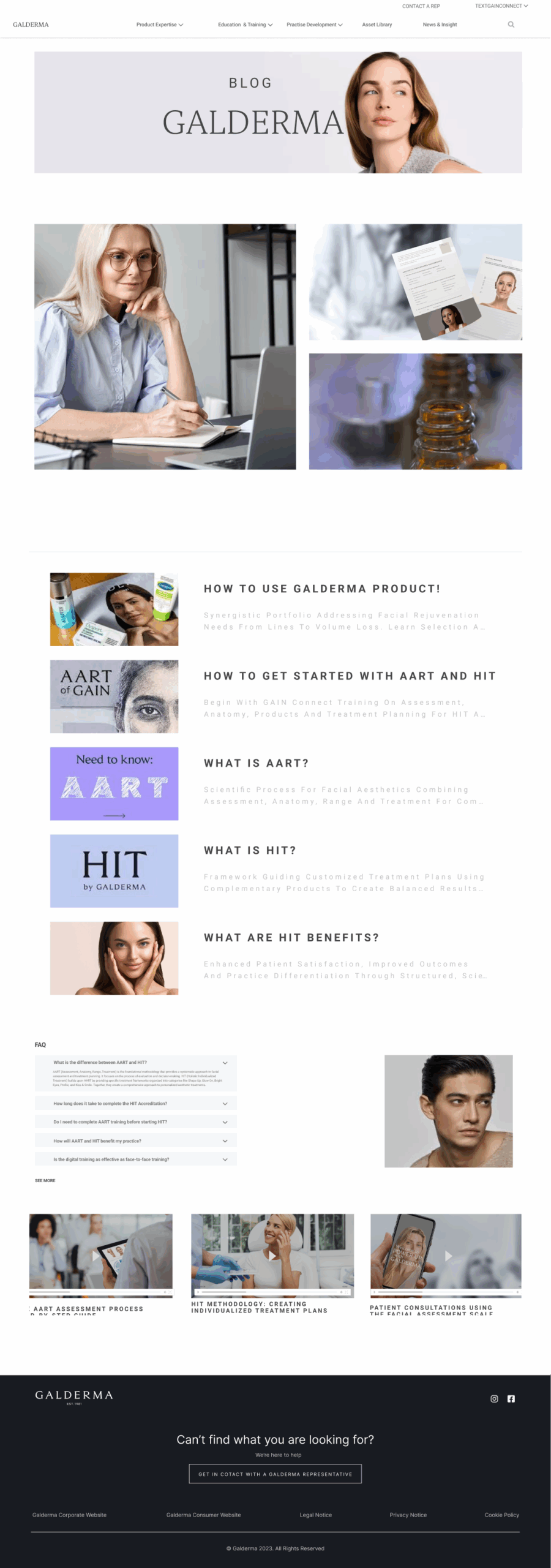
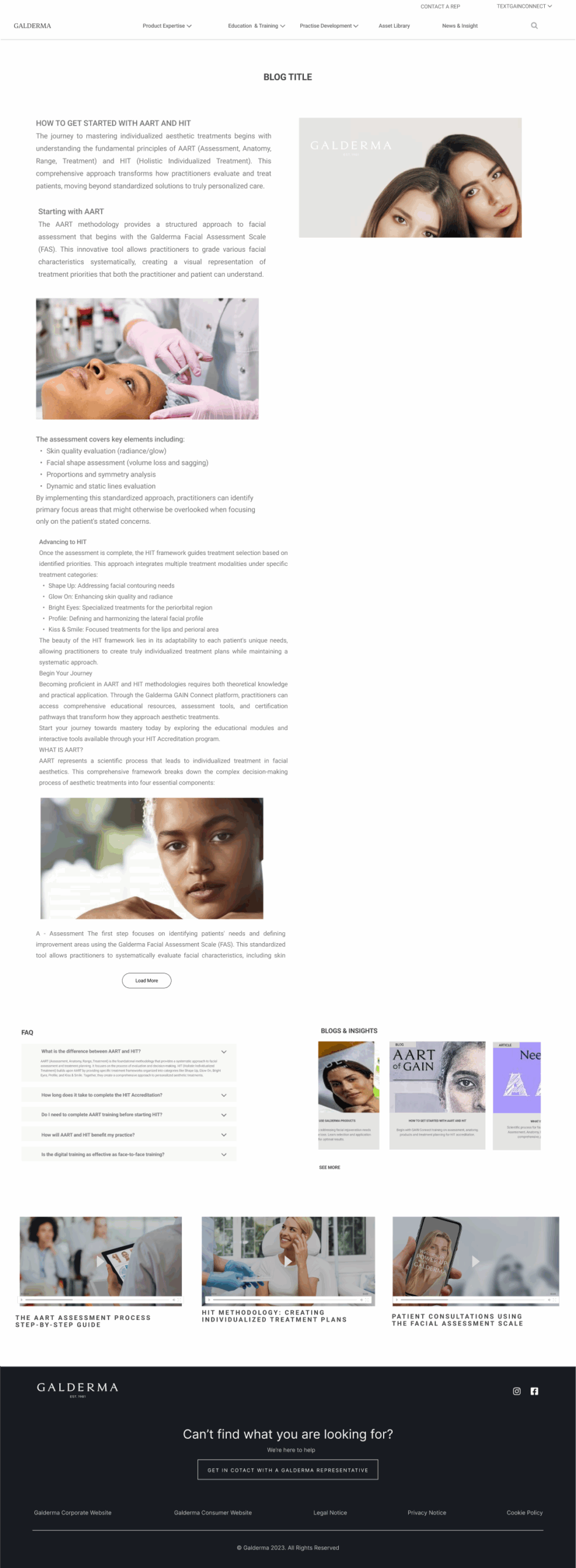
Collaborating with global educators to translate AART’s methodology into meaningful digital learning experiences. We realized that a static library of content doesn’t create clinical habits. So, we re-architected GAIN Connect using a User Engagement State framework, shifting our design goal from “organizing information” to “engineering milestones.” This strategy dictated a new Experience Design architecture: we moved from an open-access model to a Gated Progression System that forces users through specific behavioral thresholds.
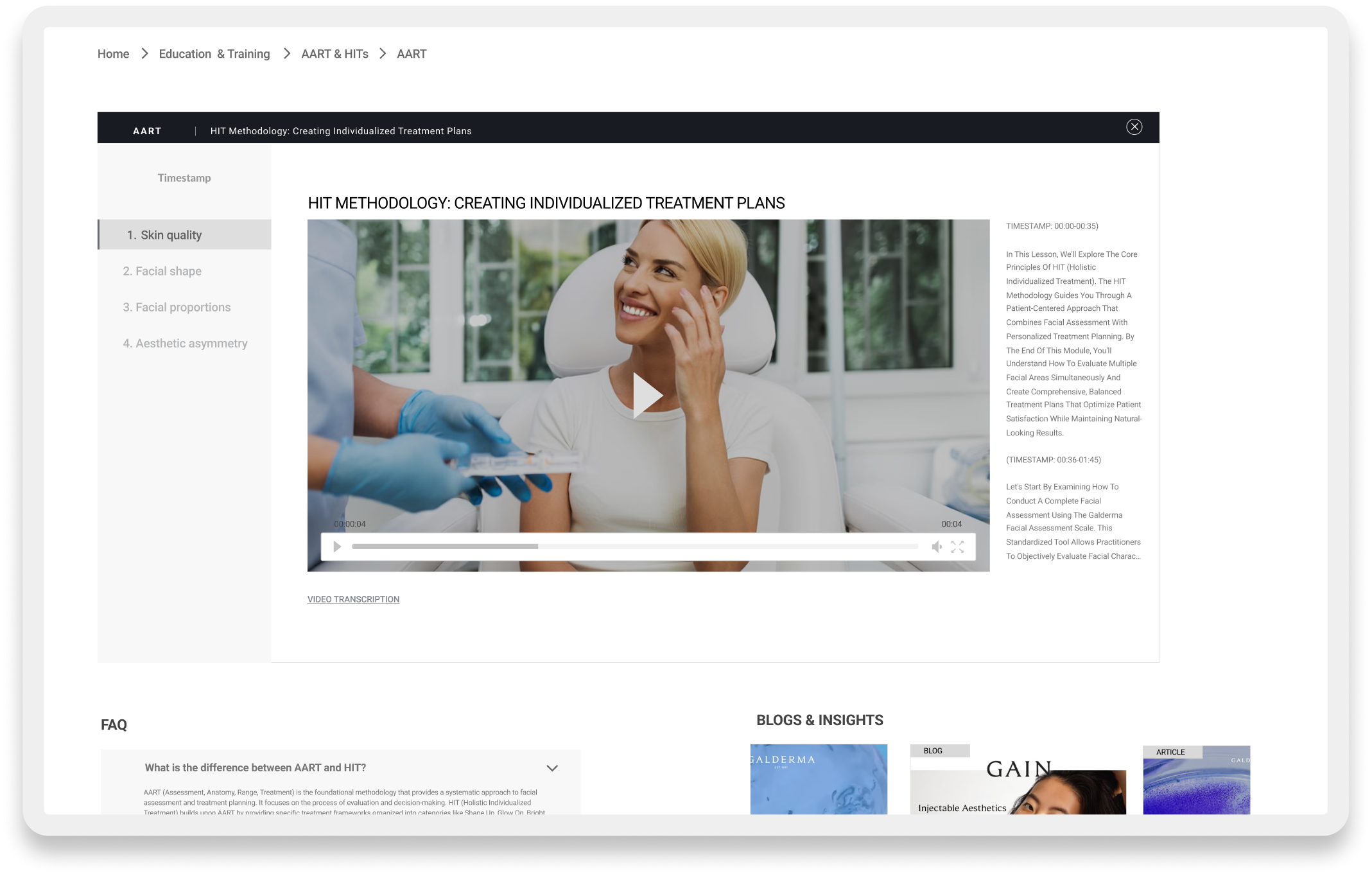
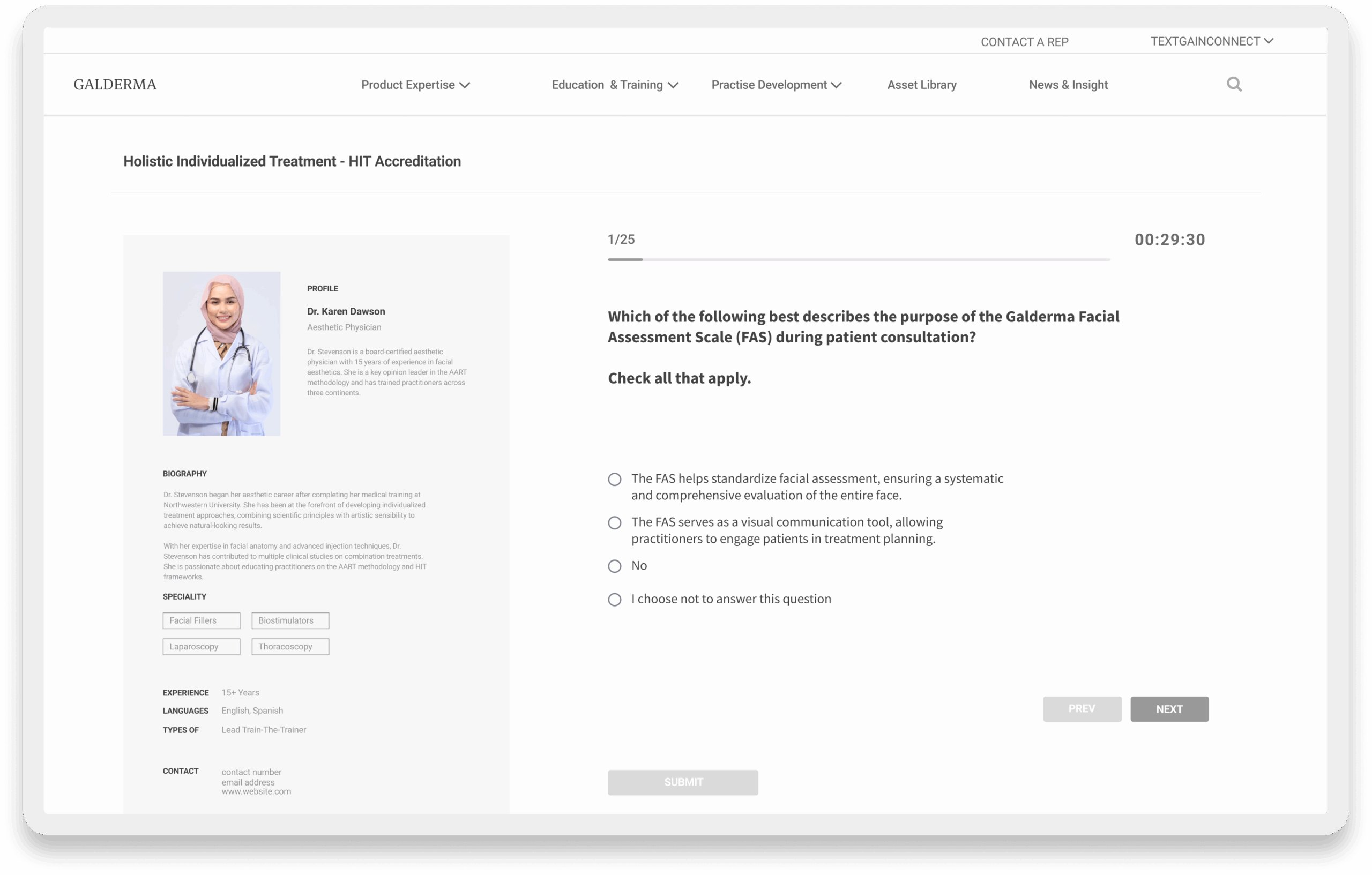
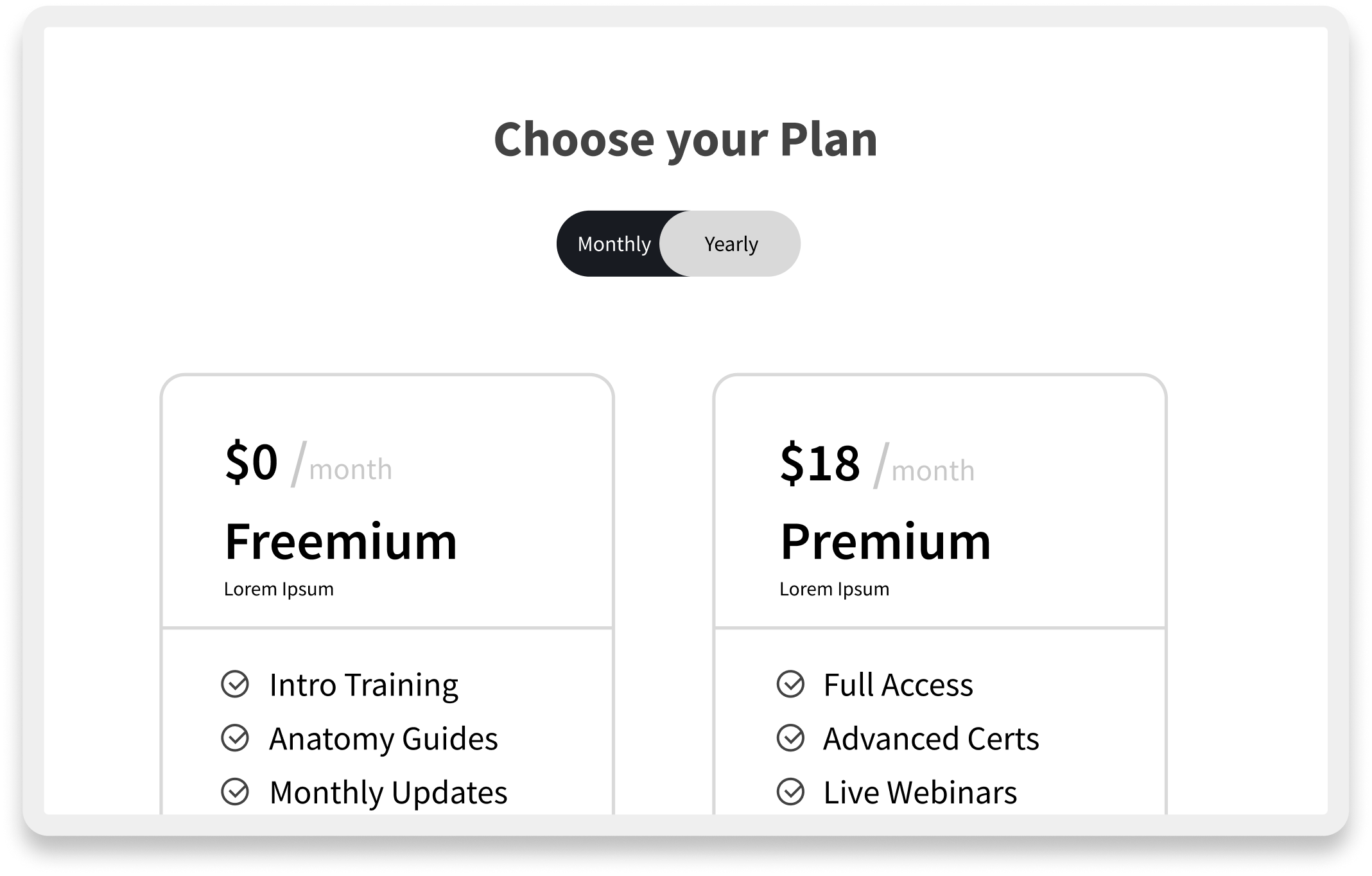
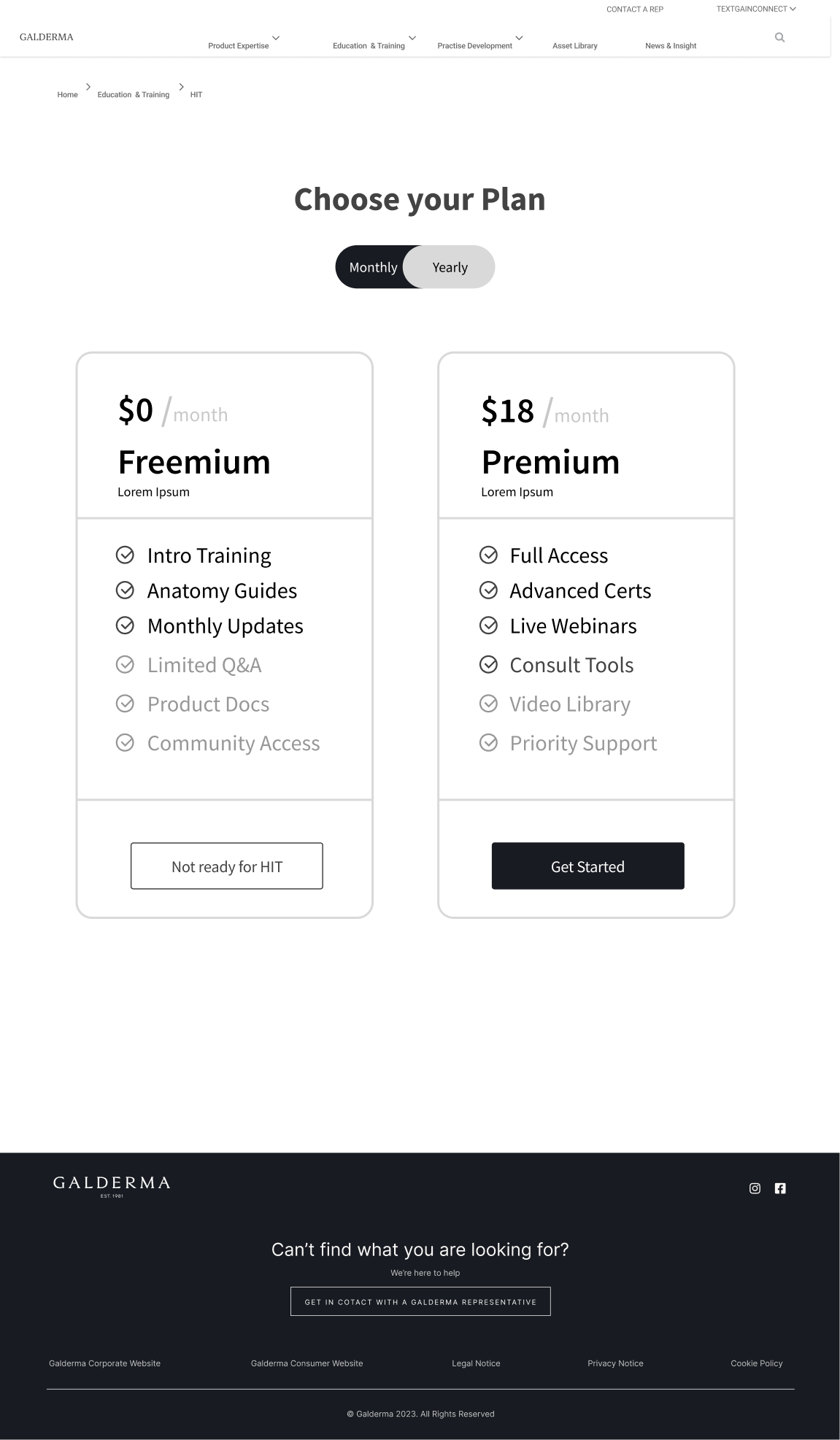
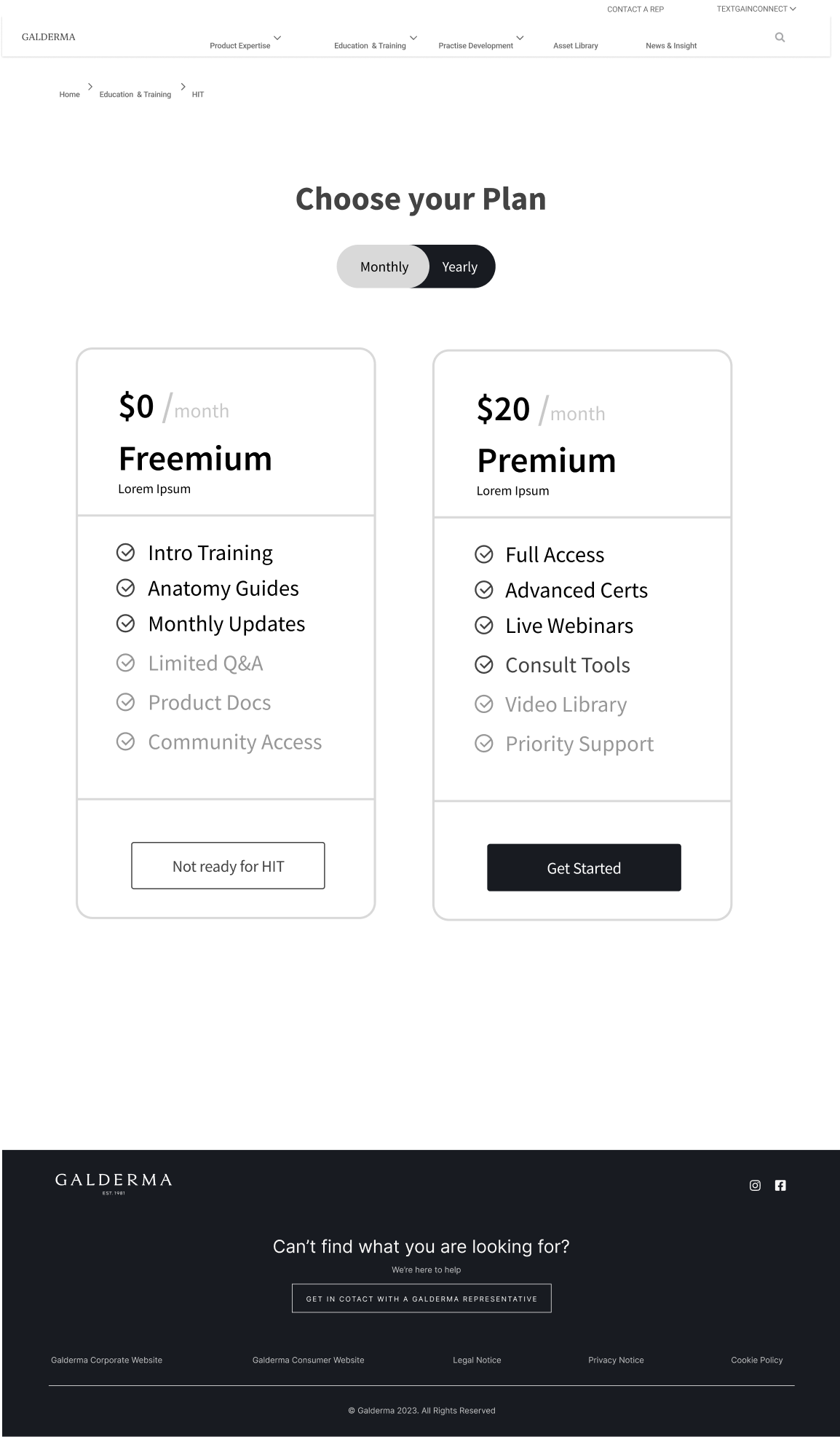
This slider demonstrates three key engagement features: timestamped video modules that enable 'Smart Resurrection' by directing users who fail assessments back to specific lessons instead of restarting entire courses; the Interactive Facial Assessment Scale (FAS) that serves as the 'Aha!' moment where users experience core clinical value through active diagnosis; and the tiered plan interface that forces active commitment between Freemium and Premium, eliminating passive 'Non-Activated' user states.
Toolkit, Methods & Frameworks
Collectively, the team and i created a robust library of strategic artifacts to align the organization around the PLG model, establishing a single source of truth for both the clinical methodology and the digital experience. Here are some of the assets below, and not limited to.
Higher Completion Course completion rates surged
indicating a successful transition from “Activation” to “Habit”.
Engagement
Interactive modules drove triple the engagement, moving users from “Casual” to “Core” states.
Confidence in HCPs
Pilot participants reported significantly higher confidence, validating the effectiveness of the “Aha! Moment” across 2 global markets.
Reflections & Impact
We started with a vision to democratize premium aesthetic education, moving from a scarcity model to a Product-Led Growth engine. To validate this shift, we moved beyond vanity metrics and focused instead on the User Engagement States mapped in our KPI tree. The data confirmed the strategy: we achieved a 45% increase in course completion (retention) and a 3.2x lift in engagement (Power User depth). By engineering the “Habit Moment”, we established a cost-efficient engine for market leadership, likely driving a 15–25% uplift in product adoption by ensuring users were clinically active, not just digitally registered. This approach operationalized education, turning the GAIN Connect platform into an engagement engine that moved practitioners from “Casual” learners to “Power” users, securing Galderma’s position as the primary architect of aesthetic education worldwide.
Next Steps
- Enhance Resurrection: Automate the “Hail Mary” loops with AI-driven content recommendations based on specific failure points.
- Deepen Power Usage: Expand the Clinic Management module to include patient scheduling, increasing platform stickiness.
- Automate Verification: Use AR to act as a “digital supervisor” for the Habit Moment, reducing reliance on human oversight.
- Social Proof Loops: Integrate peer success stories into the Setup Moment to increase Activation velocity.

