Overview
The OC Navigator is a digital platform designed to streamline connections between Orange County residents and mental health resources. By integrating physical, mental, and social health factors, the platform drives equitable access. It reduces crisis response times and transforms a fragmented system into a coordinated care network that sees the whole person, not just a patient. In Orange County, over 650,000 adults need mental health or substance abuse support, yet only 59% actually receive the care they need. This disparity represents a fractured landscape where vulnerable populations face linguistic barriers, stigma, and a maze of disconnected agencies. The system was fragmented, forcing residents to retell their trauma repeatedly just to find a door that opened. Working alongside CalMHSA, the Orange County Health Care Agency, and UCLA, I led the design and research for the OC Navigator. This was a participatory design effort to build a digital platform integrating social determinants of health (SDoH). We aimed to reduce crisis response times and drastically improve referral accuracy by moving from isolated touchpoints to a whole-person journey, making help-seeking more intuitive and dignified.
Research & Design
Participatory Design Research · Product Design · Accessibility & Privacy Compliance · Prototyping · Journey Mapping User Research · Stakeholder Collaboration
- Duration: 2022
- Partners: CalMHSA, Orange County Health Care Agency, UCLA
- Team: Fas Lebbie, Kris, Bowen Chung, Minhxuan Tran
Confidentiality: Details have been adapted to protect sensitive information while showcasing my design approach.

What I Brought
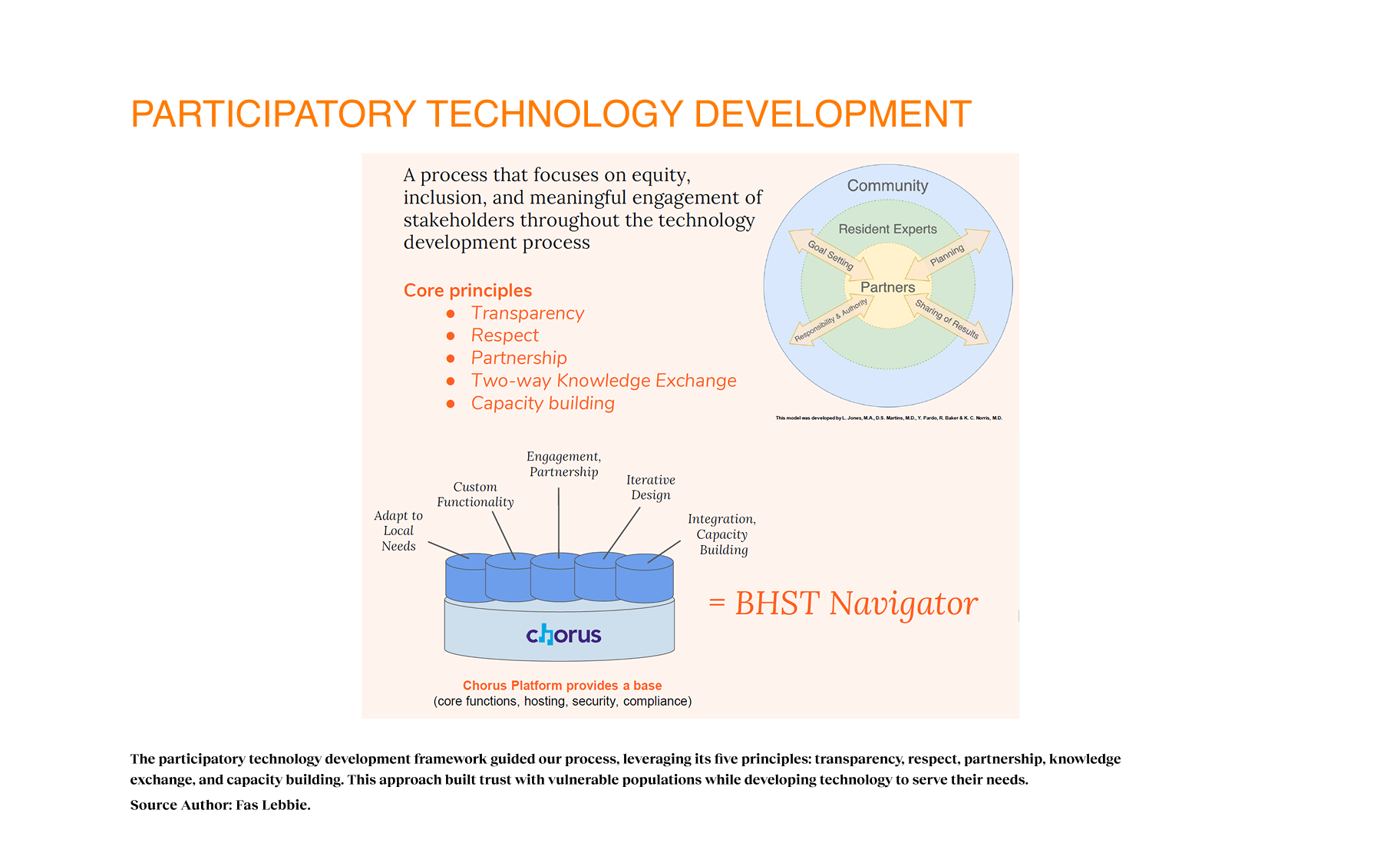
I led co-design sessions and structured interviews with 119 community members and stakeholders across 13 workgroups, utilizing a participatory technology development approach that ensured equity and inclusion drove the design vision. I integrated values of transparency and partnership, shifting our mindset from building for a community to building with them. The lived experiences and insights guided the methods and frameworks I employed, ensuring we solved for human realities. This qualitative analysis revealed the "hidden" barriers, such as stigma and cultural nuance, that data alone could not detect.
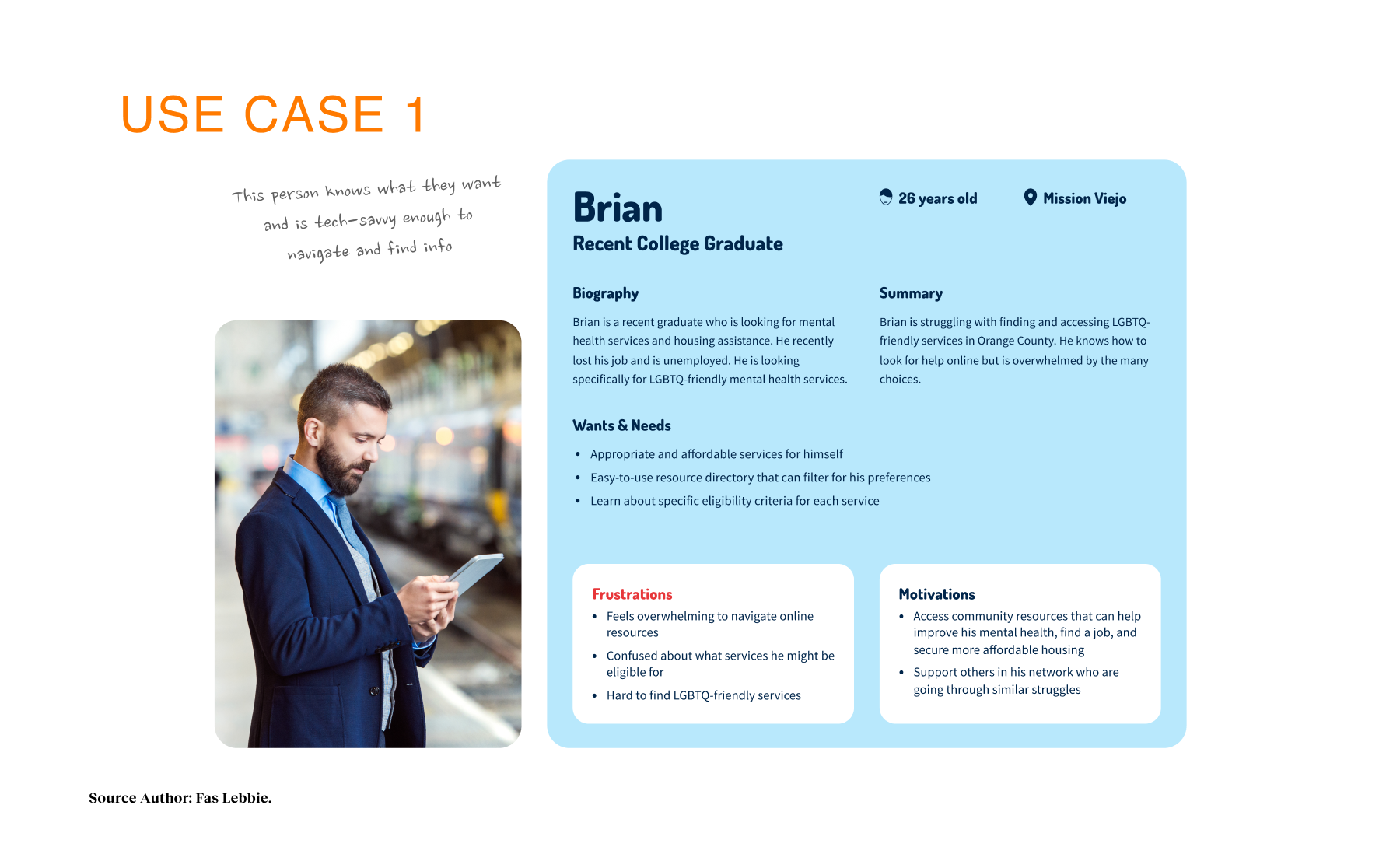
I designed accessible mobile and web interfaces, using archetypes such as "The Explorer" and "The Techie" to guide feature development. By connecting data to design outcomes, I helped improve the experience design for recovery-oriented outcomes. I worked closely with IT security teams to navigate complex compliance requirements, including WCAG and HIPAA-aligned practices, ensuring our "trusted vendor" status without compromising user experience, speed, or accessibility.
Problem Context
20.7% of Orange County adults, which equates to over 650,000 neighbors, required mental health support, yet barely half were getting it. COVID-19 had only deepened these cracks, amplifying anxiety, isolation, and housing insecurity. But the real issue was not just scarcity. It was opacity. As resource hubs shifted to virtual formats, they inadvertently erected new barriers for those with limited digital literacy, transportation challenges, or language barriers.
The fragmented nature of the system meant a user might have to navigate multiple agencies, repeating their story over and over, effectively traumatizing them in the search for relief. Public and private behavioral health systems lacked coordination, and insurance networks failed to support person-centered access. Providers were operating in silos with separate databases, some even relying on personal Excel sheets, leading to confusion and missed handoffs. We realized the current model prioritized quantity of services over the quality of the recovery journey, creating a profound disconnect between the “system” and the human needs it was meant to serve.
My Approach
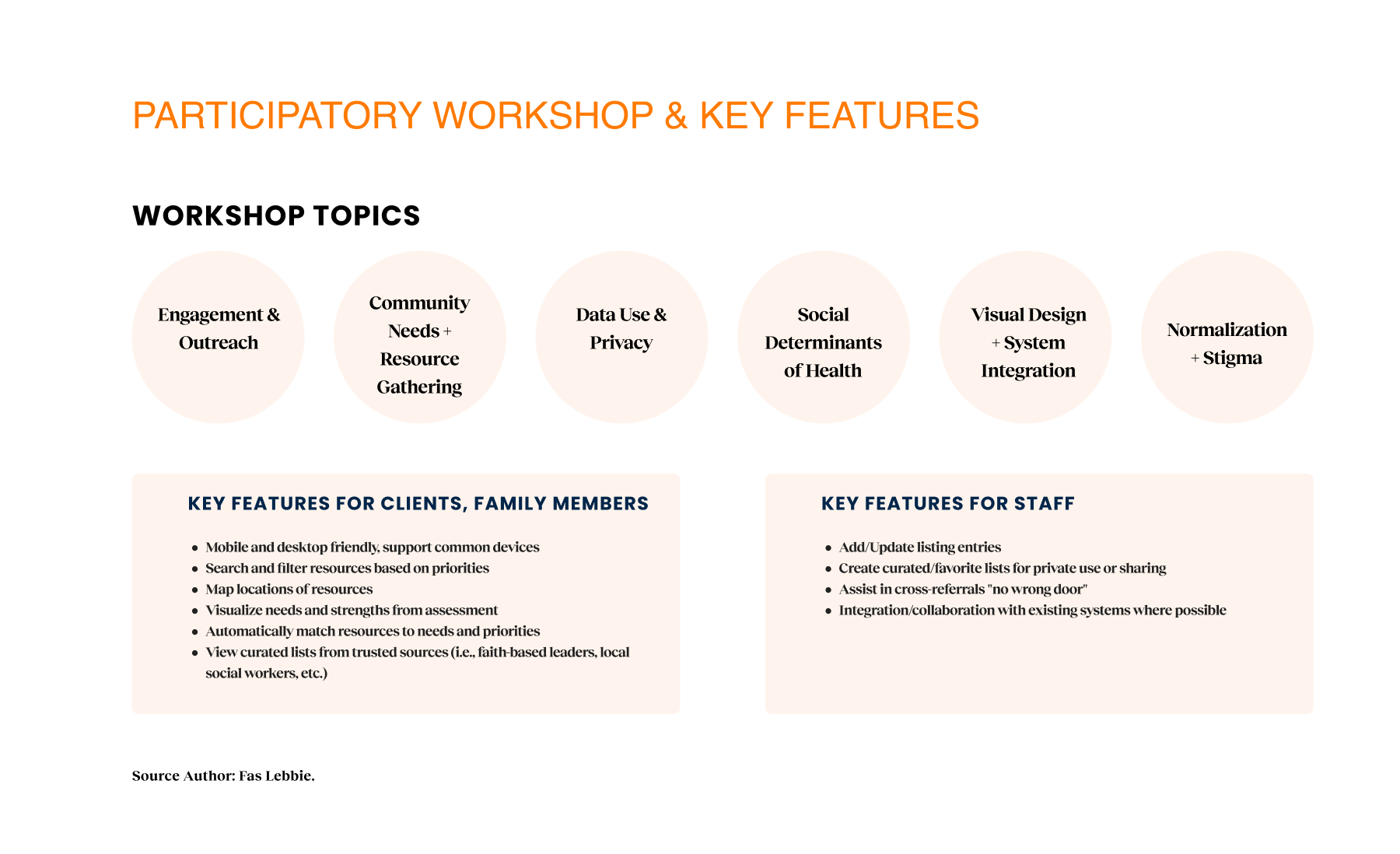
My approach centered on participatory technology development, a process that prioritizes equity, inclusion, and meaningful stakeholder engagement throughout the development process. My design process integrated core values of transparency, respect, partnership, two-way knowledge exchange, and capacity building. By engaging diverse stakeholders as partners in the development cycle, we ensured the technology responded to local needs. This participatory framework yielded a platform that addressed both practical needs and emotional barriers, effectively normalizing the process of seeking support.
Design Process
Before I formally joined, the Chorus team had laid the groundwork with focus groups, handing us a baton of raw, valuable data. It gave us a sobering starting line. We knew one in five adults needed help. We also saw clearly that traditional navigation “solutions” were failing diverse populations, particularly those facing linguistic hurdles or complex social determinants of health. Geography and insurance status were acting as gatekeepers. But the most daunting baseline reality was the cultural stigma that discouraged people from even raising their hands. We were not just designing a directory. We were designing to address systemic exclusion of monolingual communities, older adults, and individuals with limited digital literacy. The baseline data allowed us to make informed decisions to enhance engagement rather than guess what users needed.
To tackle this complexity, I adopted a grounded theory approach, conducting structured and semi-structured interviews with 119 participants across 13 workgroups. We cast a wide net by talking to first responders, program administrators, and citizens, because a mental health crisis touches every layer of the city. These were not quick chats. These were 90-minute deep dives designed to uncover the personal stories hidden behind the statistics.
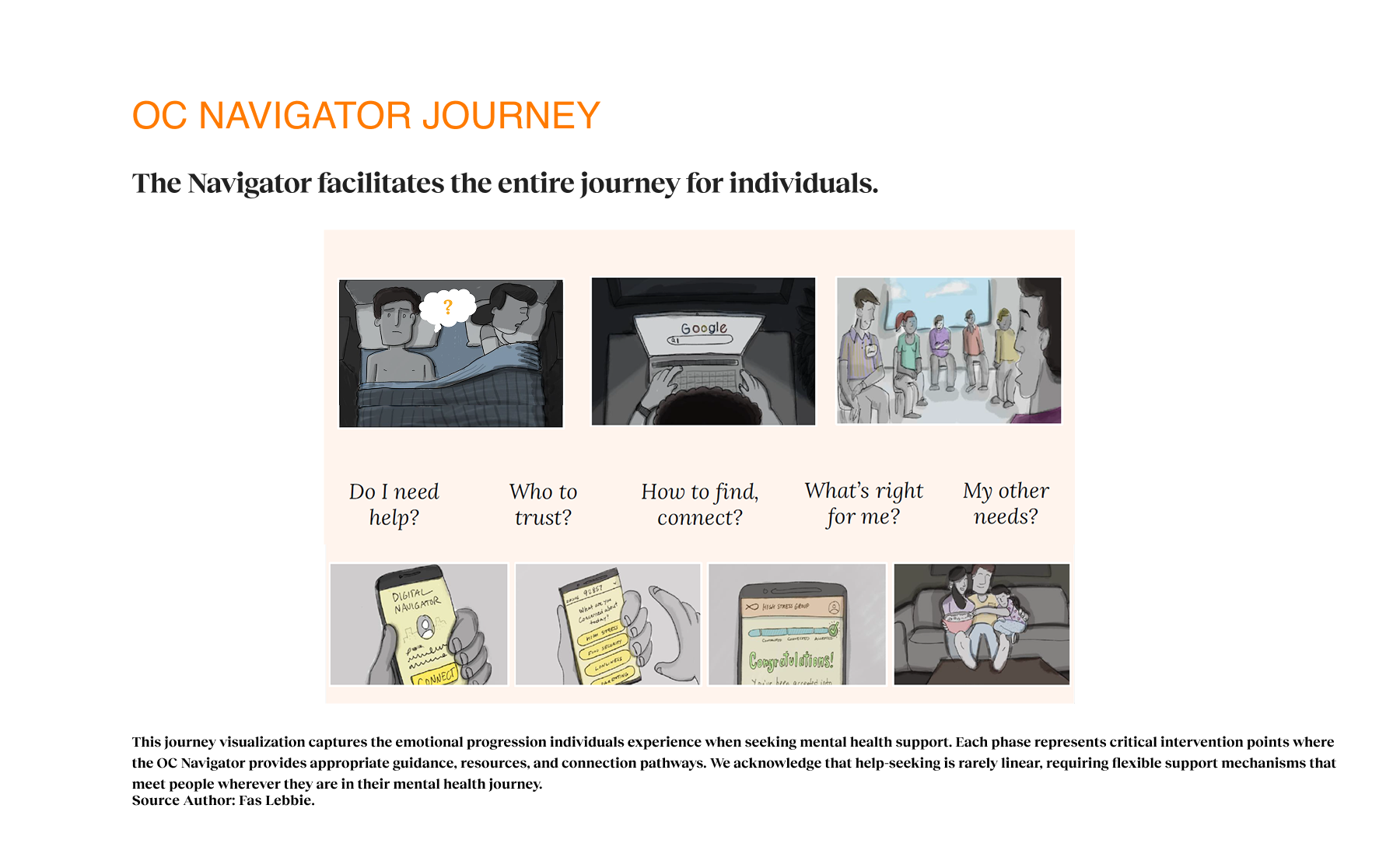
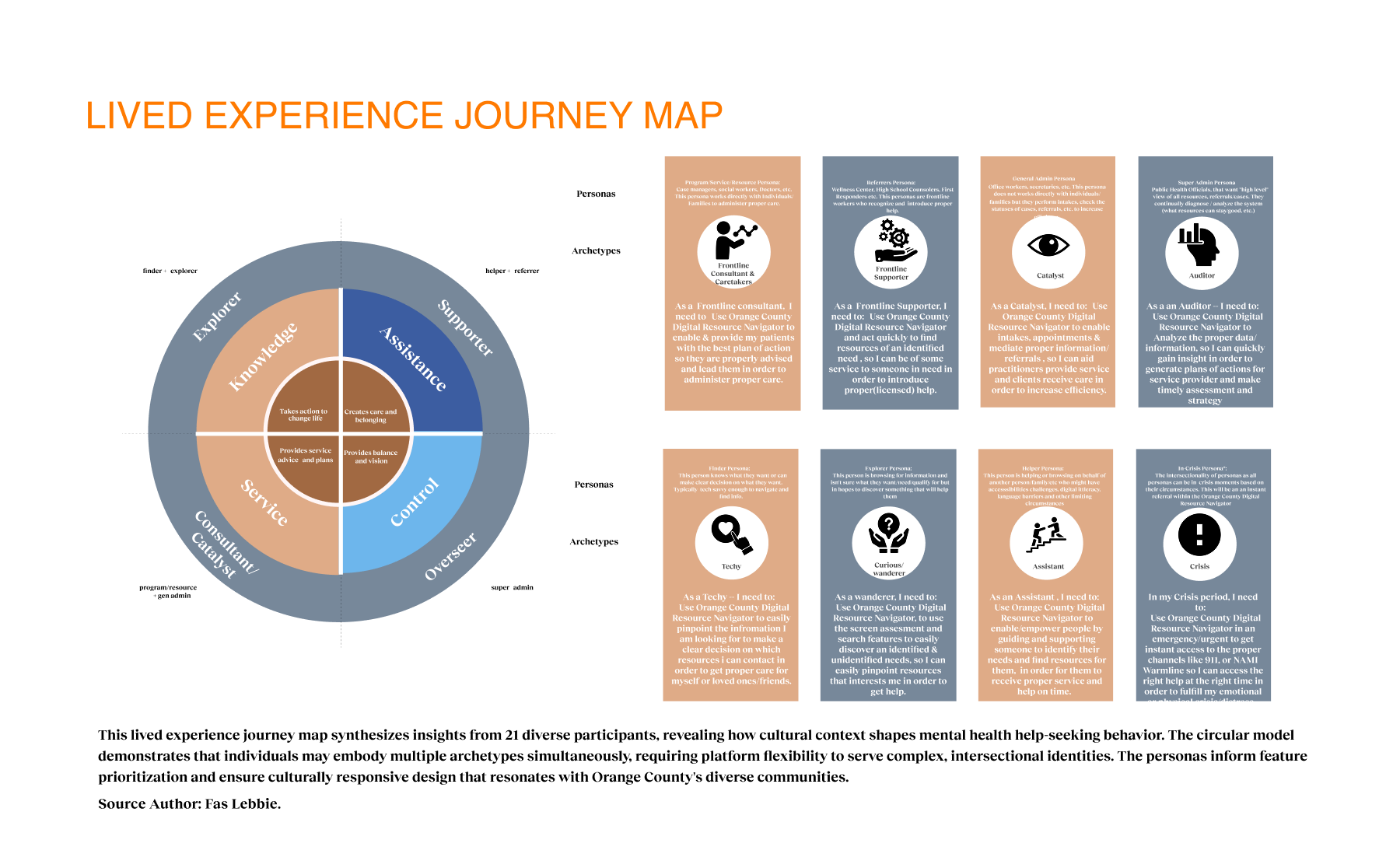
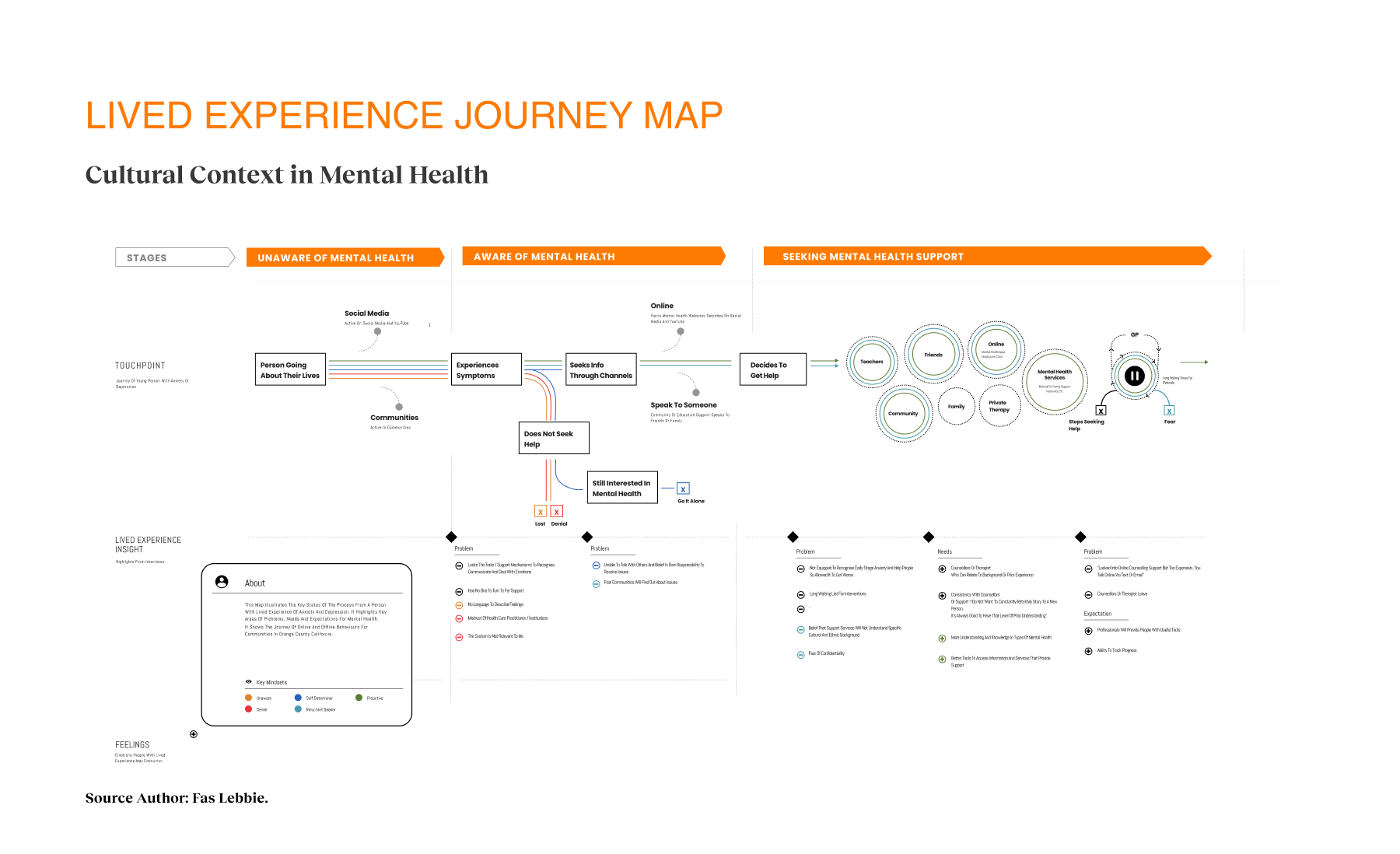
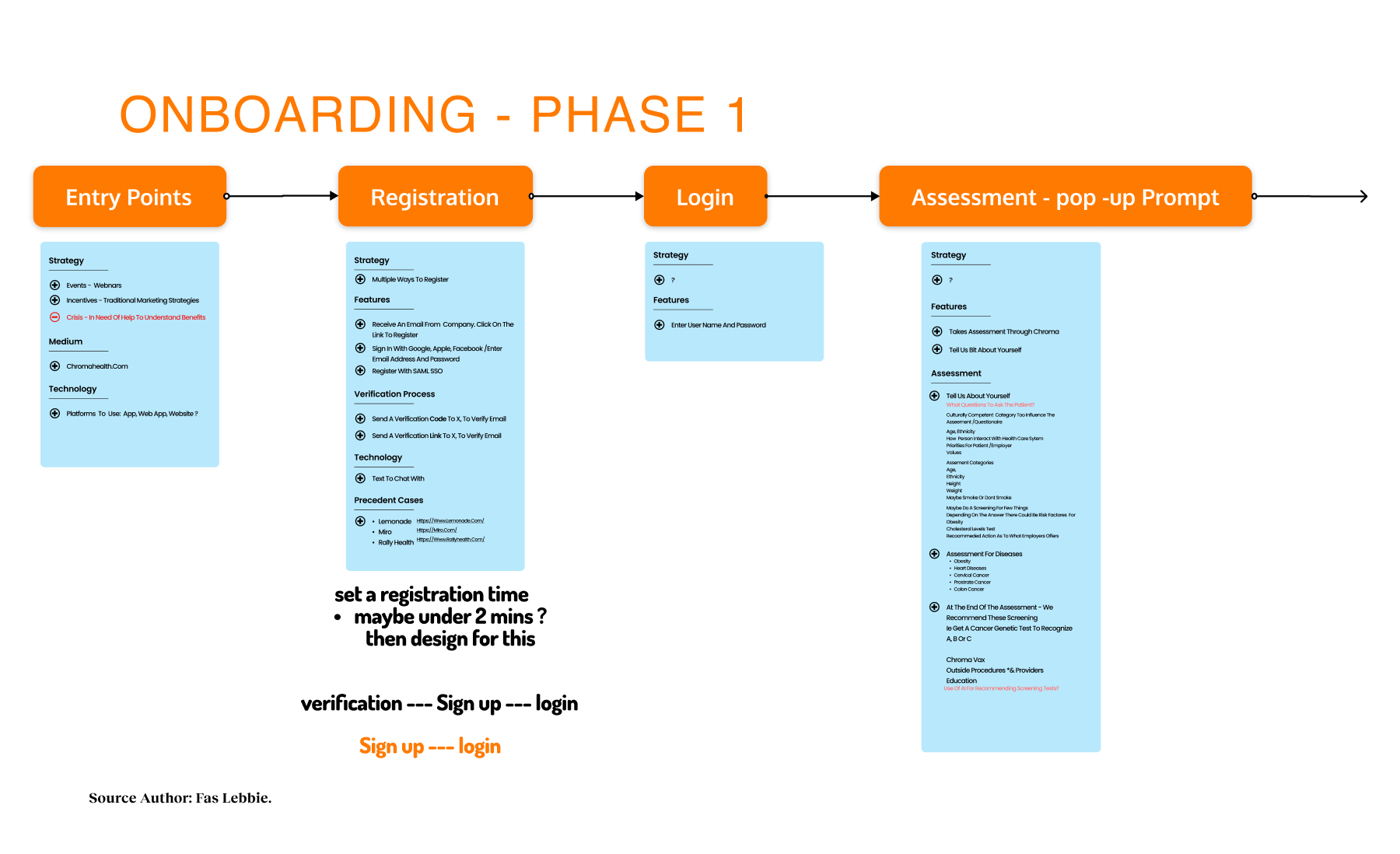
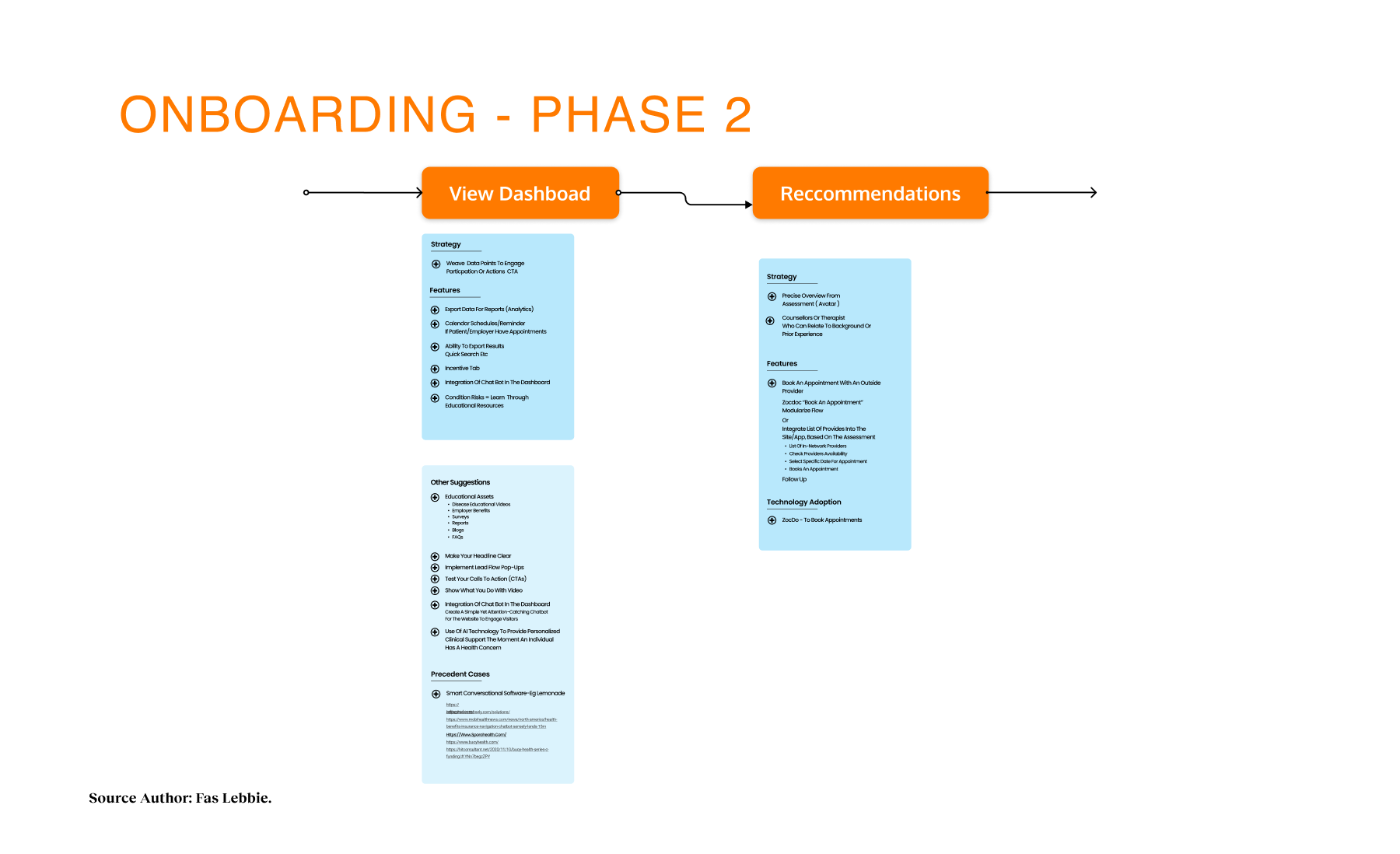
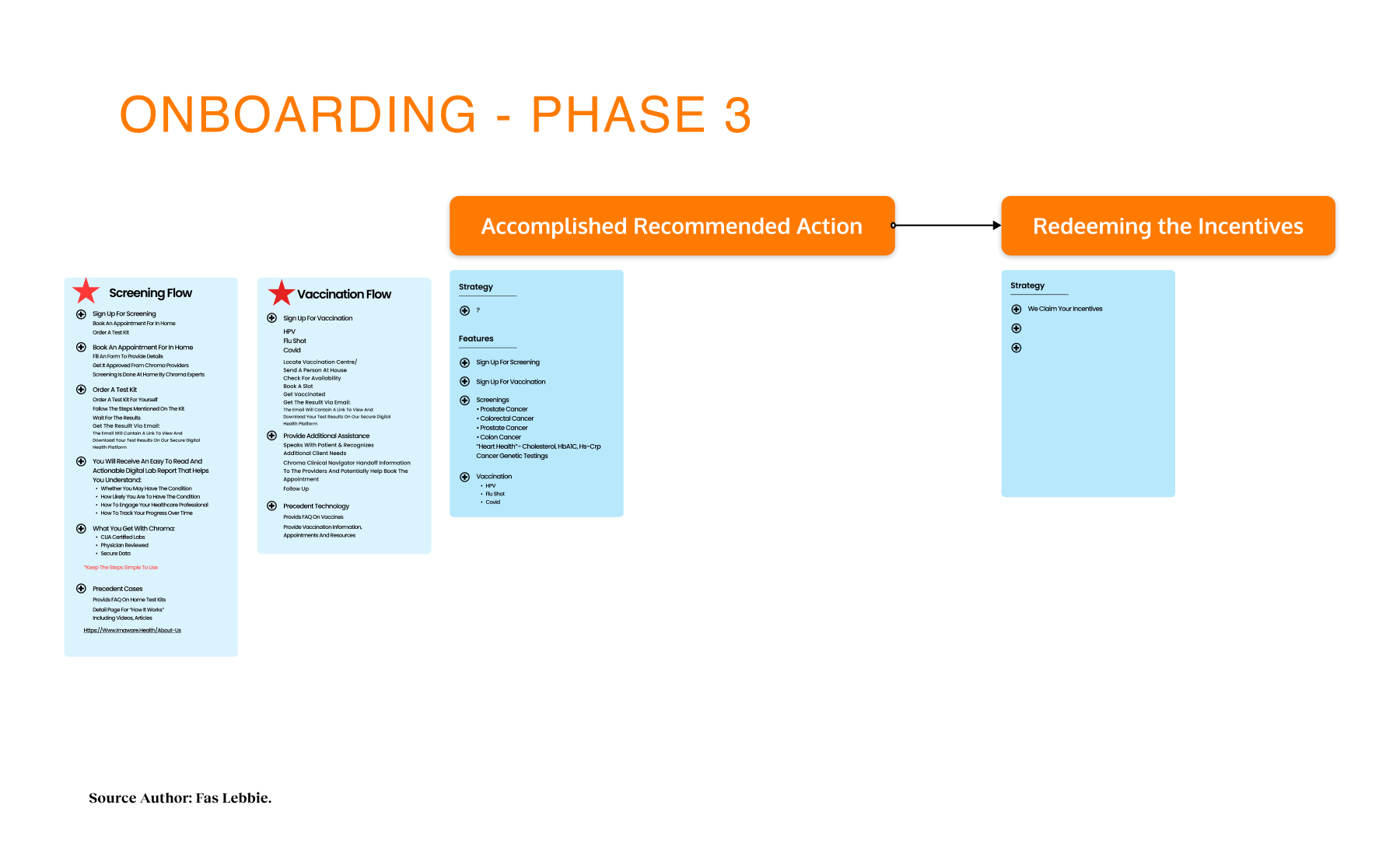
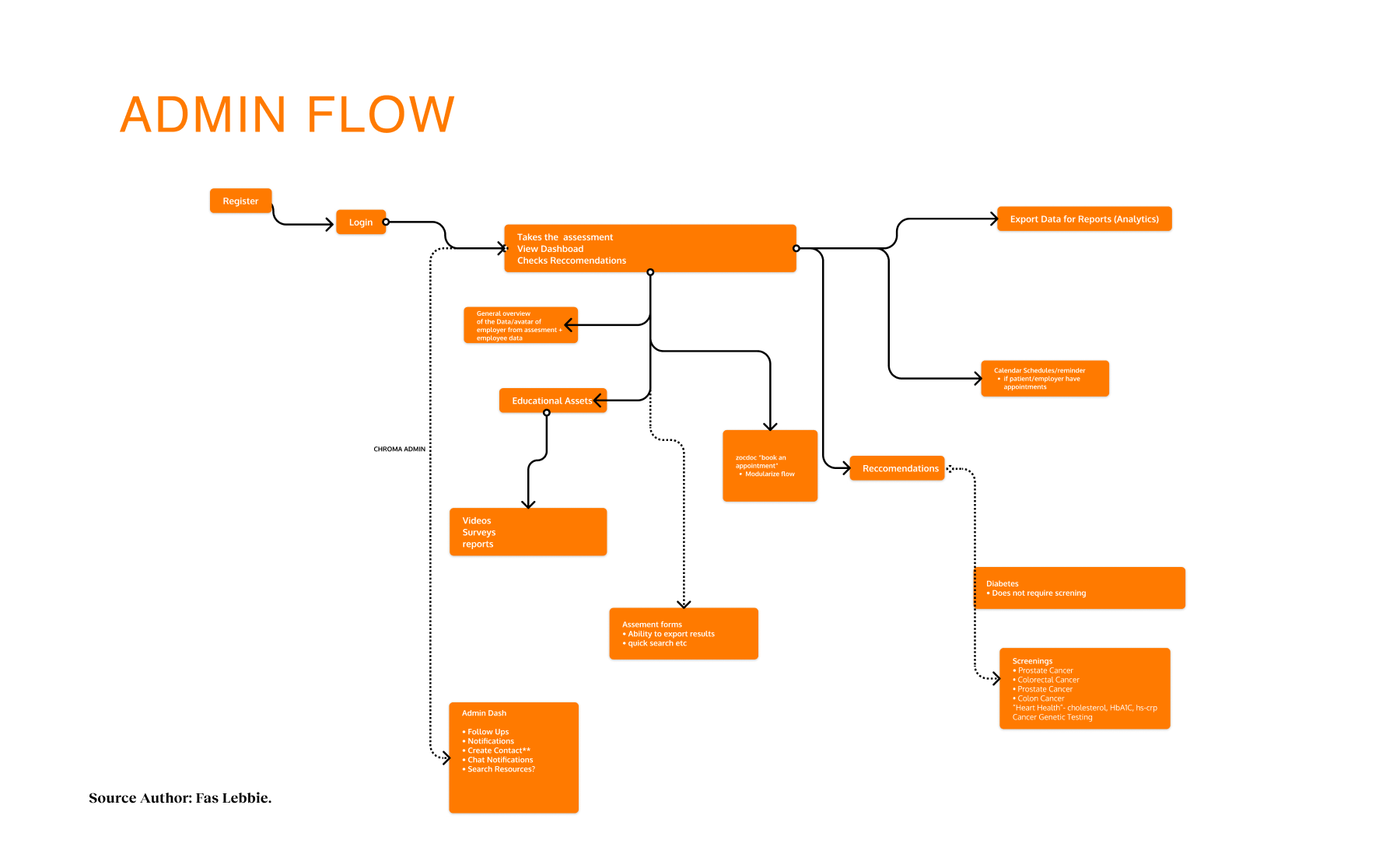
Our strategy centered on participatory technology development. Instead of building for the community, we engaged stakeholders as partners in the development cycle. We used frameworks such as the Transtheoretical Model of Health Behavior Change to map the user’s mindset from “unaware” to “proactive”. This approach revealed that social determinants, such as housing stability and food security, were just as critical as clinical therapy. We mapped the ecosystem and identified distinct user journeys, such as one for individuals seeking services and another for providers making referrals. We utilized journey maps as the key driver of our design decisions, ensuring we were solving for the “whole journey” rather than isolated touchpoints. We even developed specific archetypes, like “The Techie” vs. “The Browser,” to ensure our interface could flex to meet different cognitive styles and stress levels.
We resisted the urge to build everything at once. We proposed an MVP built on three strict requirements: usability/accessibility, SDoH integration, and data security. Before the full build, we deployed an “Alpha” version for testing to validate our core assumptions.
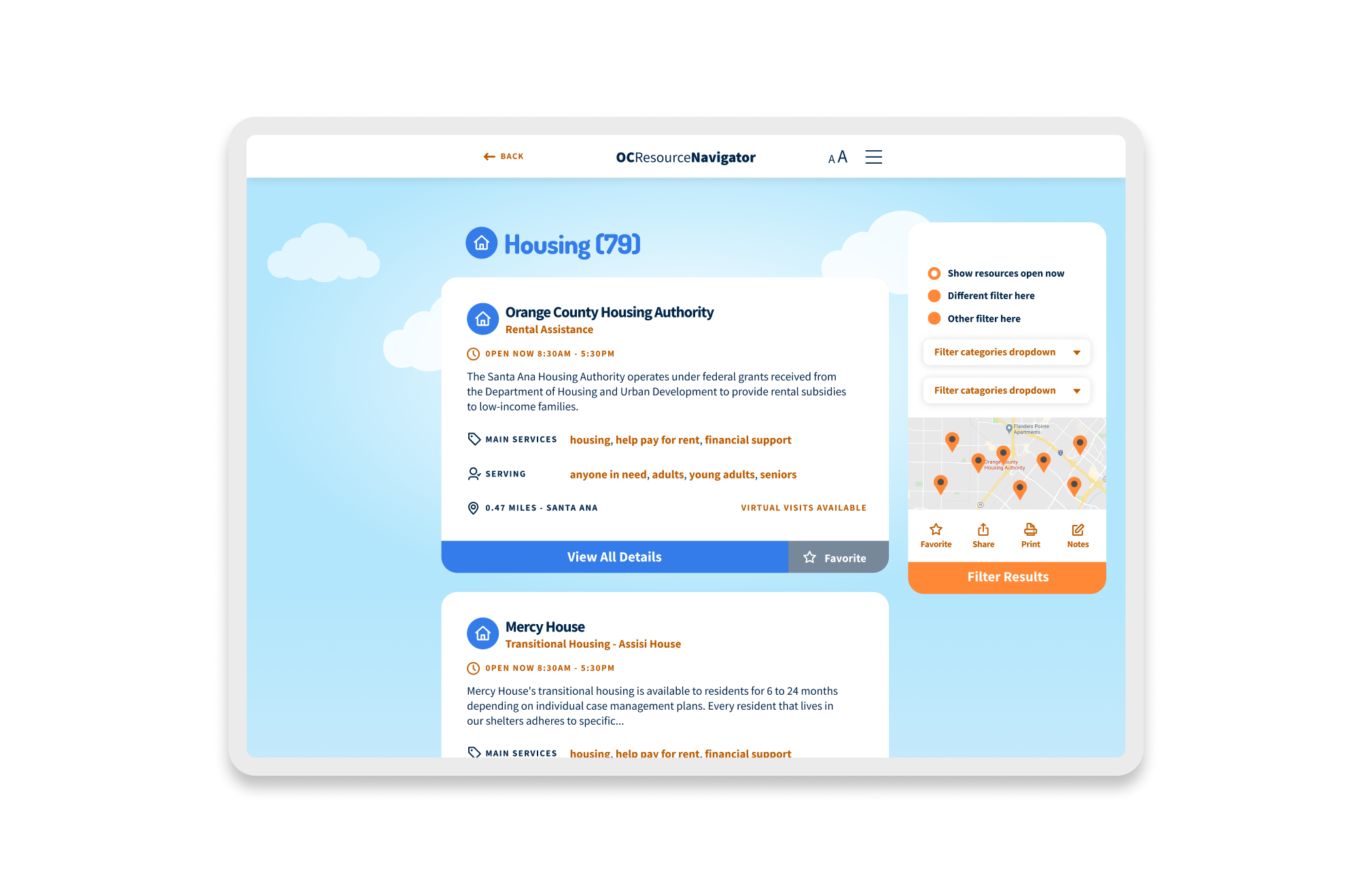
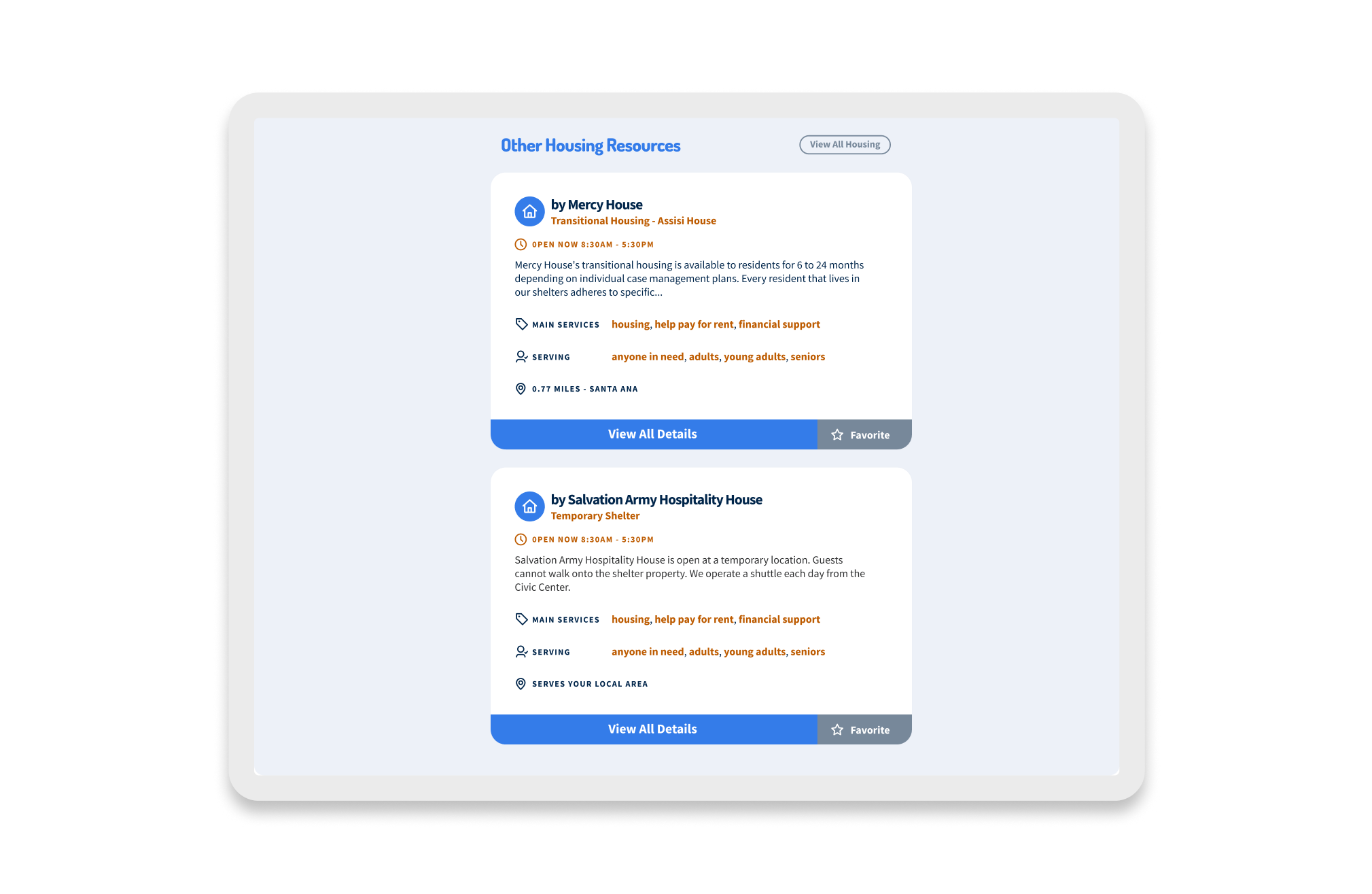
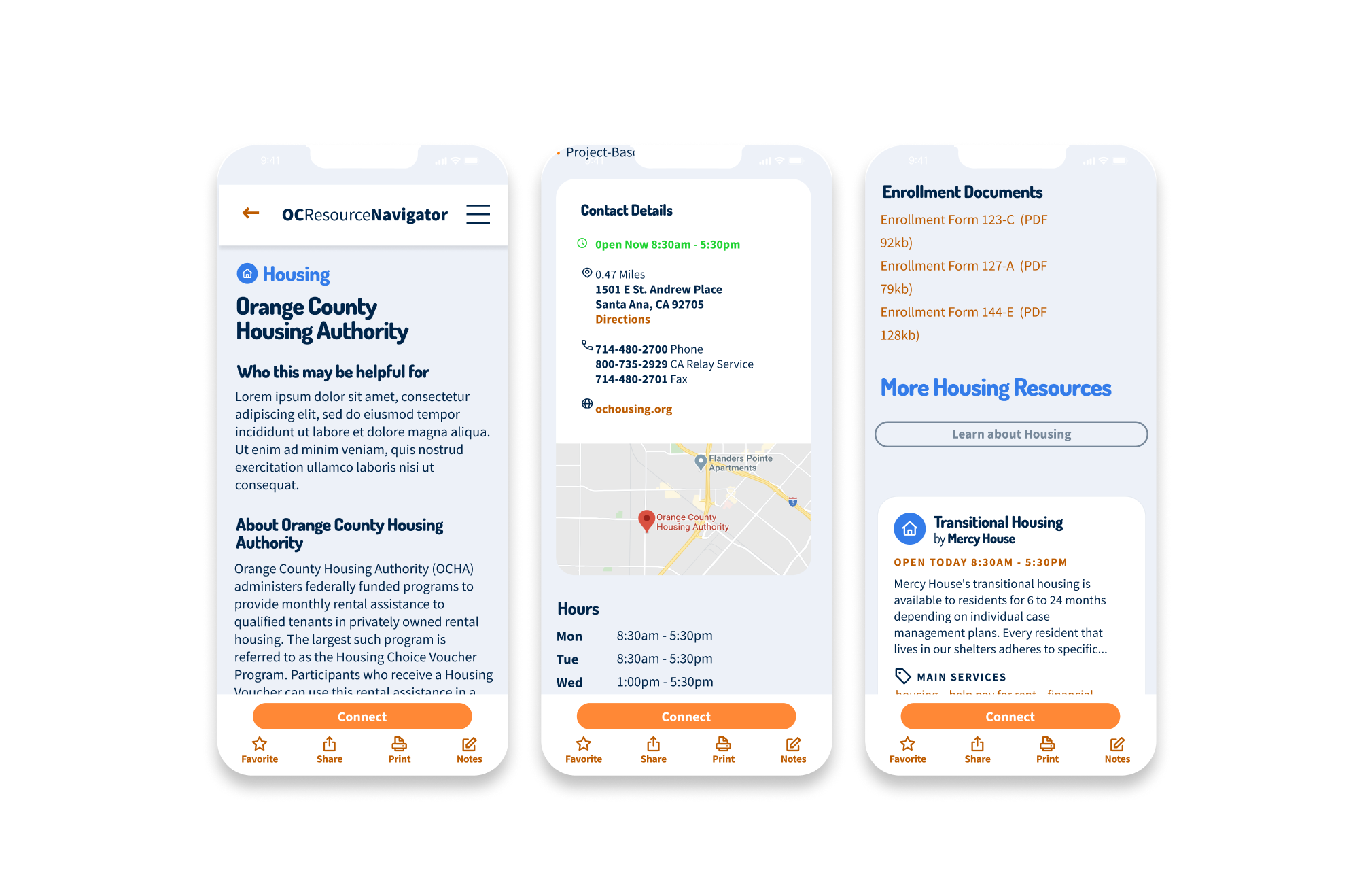
The pilot launched in March 2022, kicking off a rigorous cycle of iteration that ran through June 2022. We treated the product as a living organism. AB testing was conducted through specific user workgroups. For example, during testing of the resource listings, stakeholders rejected “Option 1,” which required an extra click to view services, preferring “Option 2,” which displayed details immediately. We listened and pivoted.
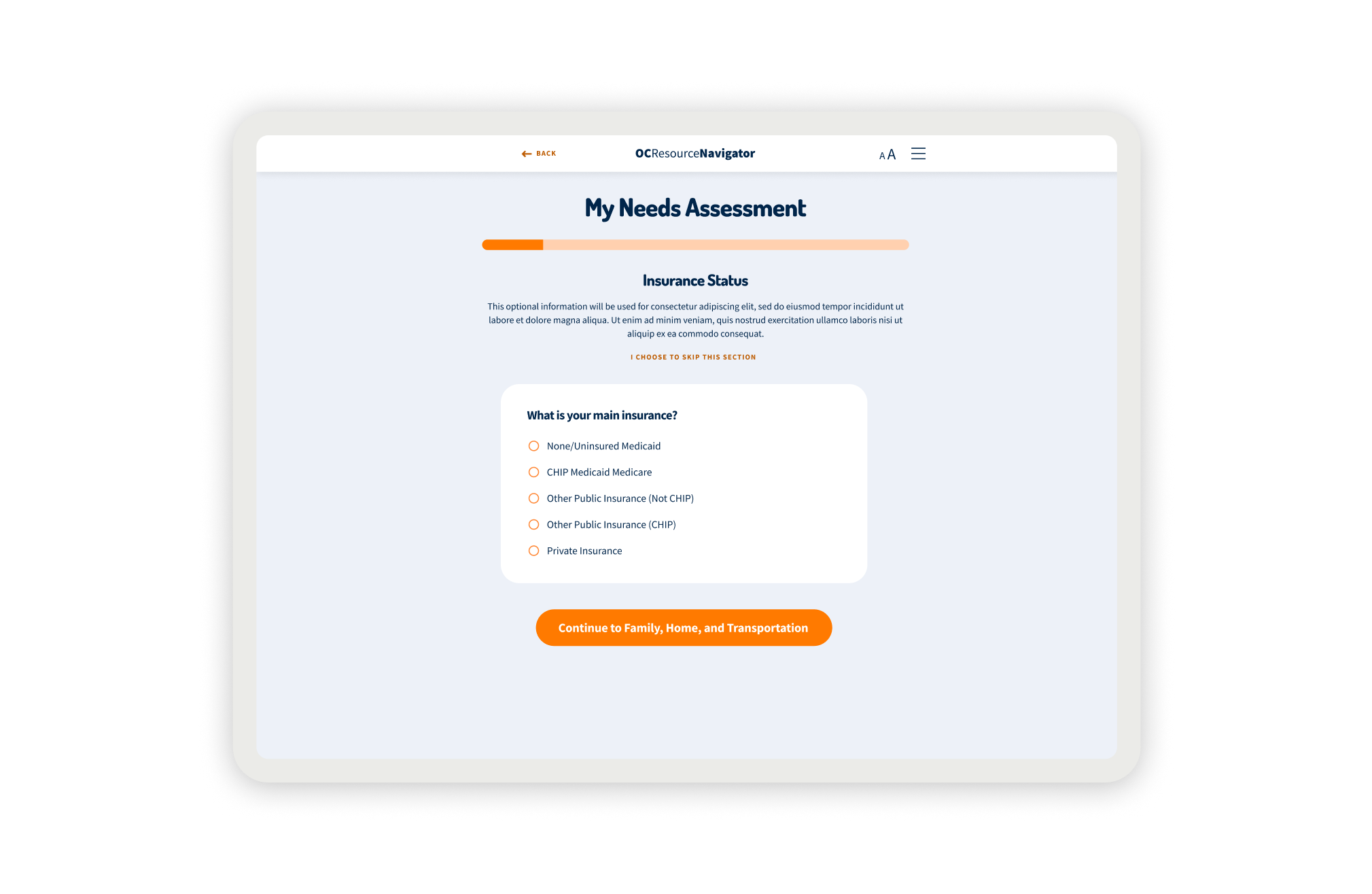
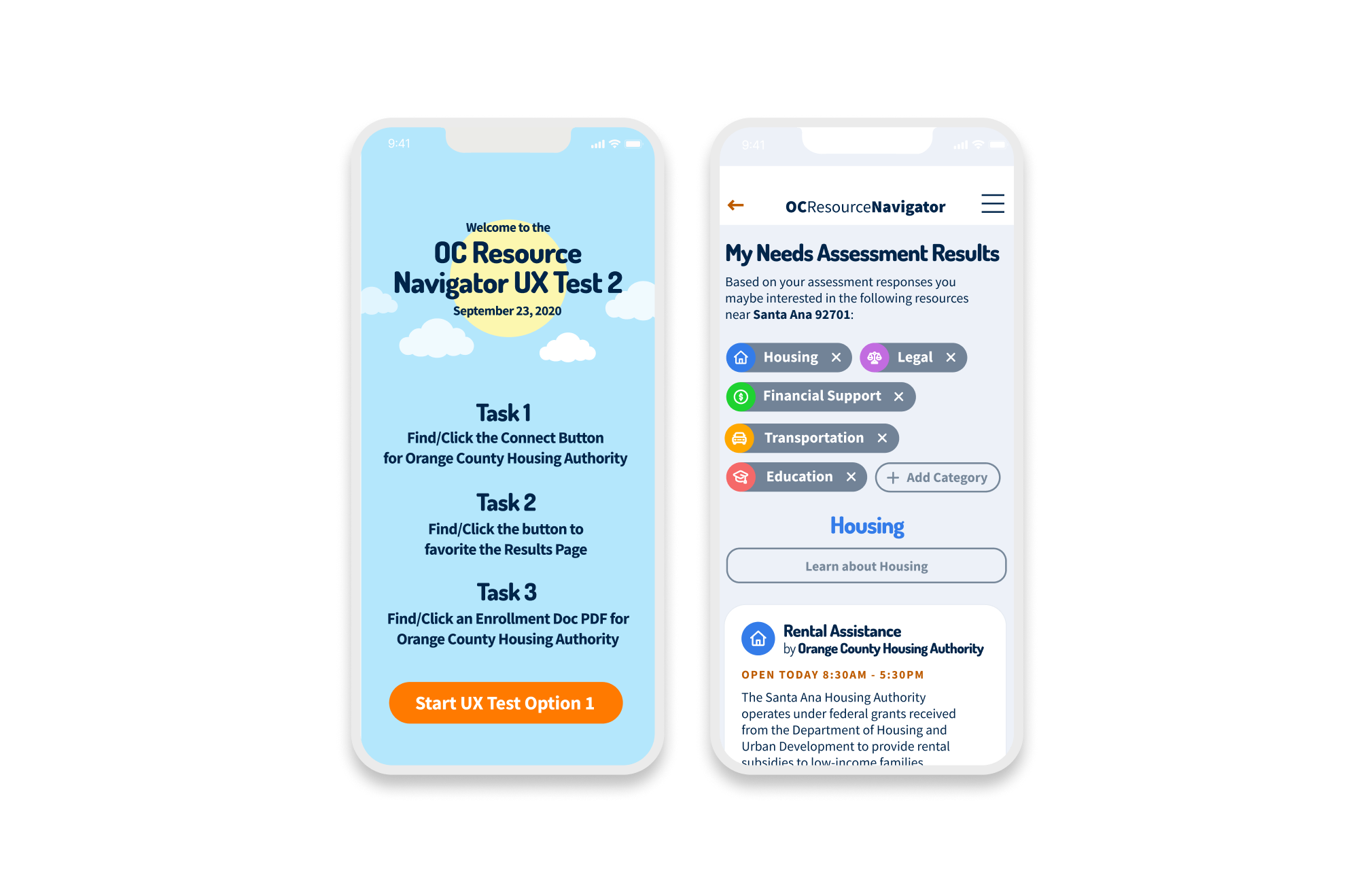
Our implementation strategy was phased. We focused first on the core functionality for individual users, such as the home page, the SDoH screener, and resource listings, before attempting the complexity of the provider dashboard and referral tracking system. Every phase was checked against user feedback, particularly regarding sensitive privacy concerns. We used tools like Maze to generate heatmaps, confirming that 76.7% of users could successfully navigate to the assessment on their first try, giving us the confidence to scale.
During our sense-making process, several pivotal themes emerged that reshaped our design criteria:
- Trust is the Gateway. Transparency is mandatory, as participants communicate the importance of service transparency in understanding who sees their data.
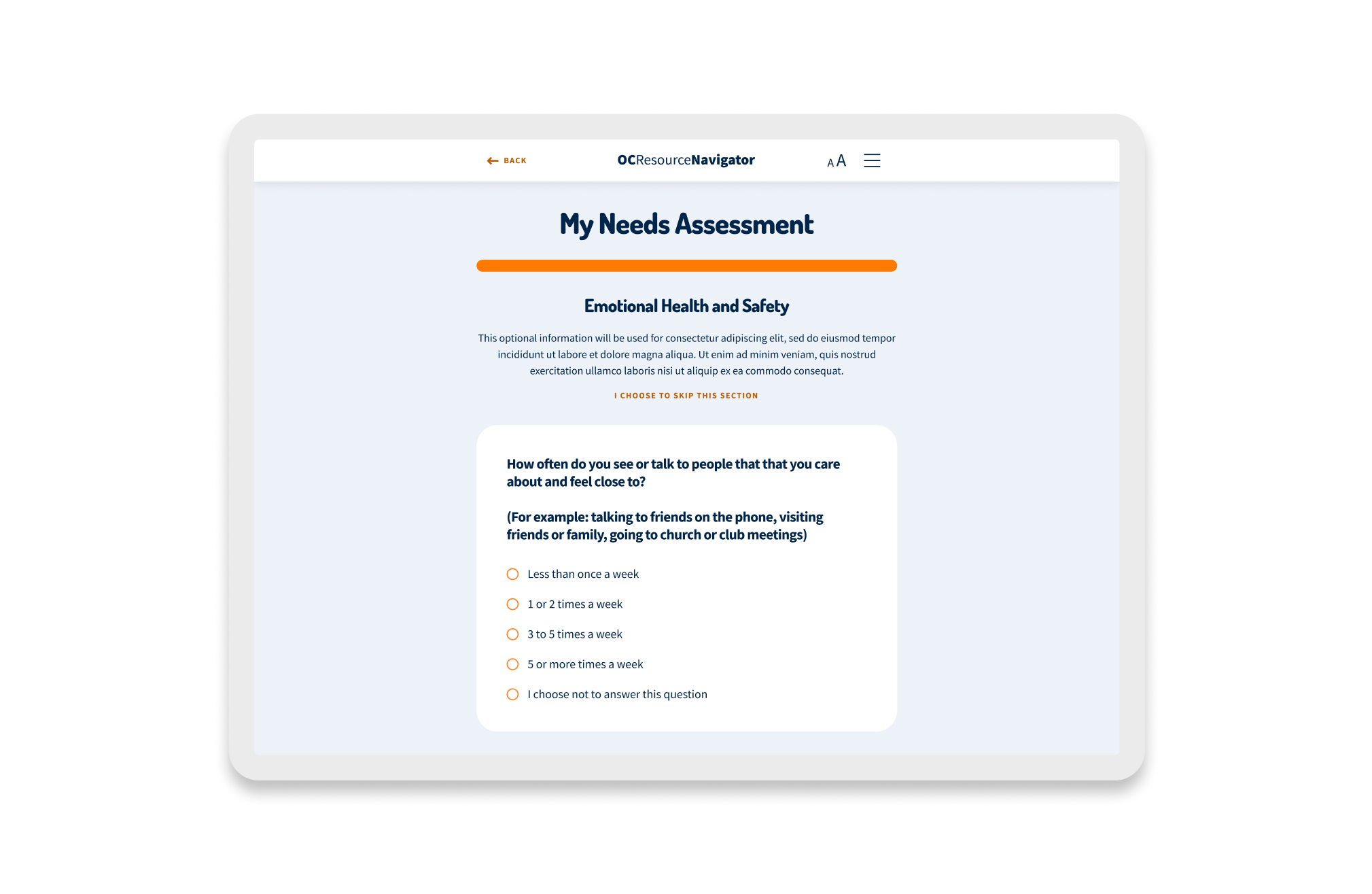
- It’s not just mental health; it’s whole-life health. Social determinants like housing stability and food security significantly affected access to services. Participants noted barriers when clients lacked phones or housing. We could not just list therapists. We integrated the SDoH screener to capture these broader needs and connect them to relevant resources, such as food pantries and housing support.
- Barriers are multifaceted. Participants reported barriers ranging from a lack of awareness to transportation and linguistic obstacles. The design needed to incorporate best practices for accessibility and address cultural stigma.
- The system is fragmented, focus on the journey. Current care is focused on quantity over outcomes. Providers were maintaining their own Excel sheets because they did not trust central lists. The platform had to focus on individual journeys rather than isolated system touchpoints, facilitating self-referrals and tracking progress so no one fell through the cracks.
The experience strategy needed to translate empathy into measurable system performance. We aligned our design decisions around three core tiers of success:
Goal: Operationalize Trust. We aimed to track engagement with the sensitive SDoH screener as a proxy for user trust and safety.
Goal: Close the Crisis Gap. The Challenge: Users in distress face an infinite loop of referrals and retold stories, often abandoning the search. The goal was to close the gap between identifying a need and receiving care, and to monitor metrics like “referral follow-through” and the reduction of “multi-contact” friction, where users had to call multiple places to get help.
Goal: System Integration. Providers relied on isolated personal Excel sheets, creating a fractured view of available care. We aimed to track the unification of disparate databases into a single source of truth to drive the $18M transformation initiative.
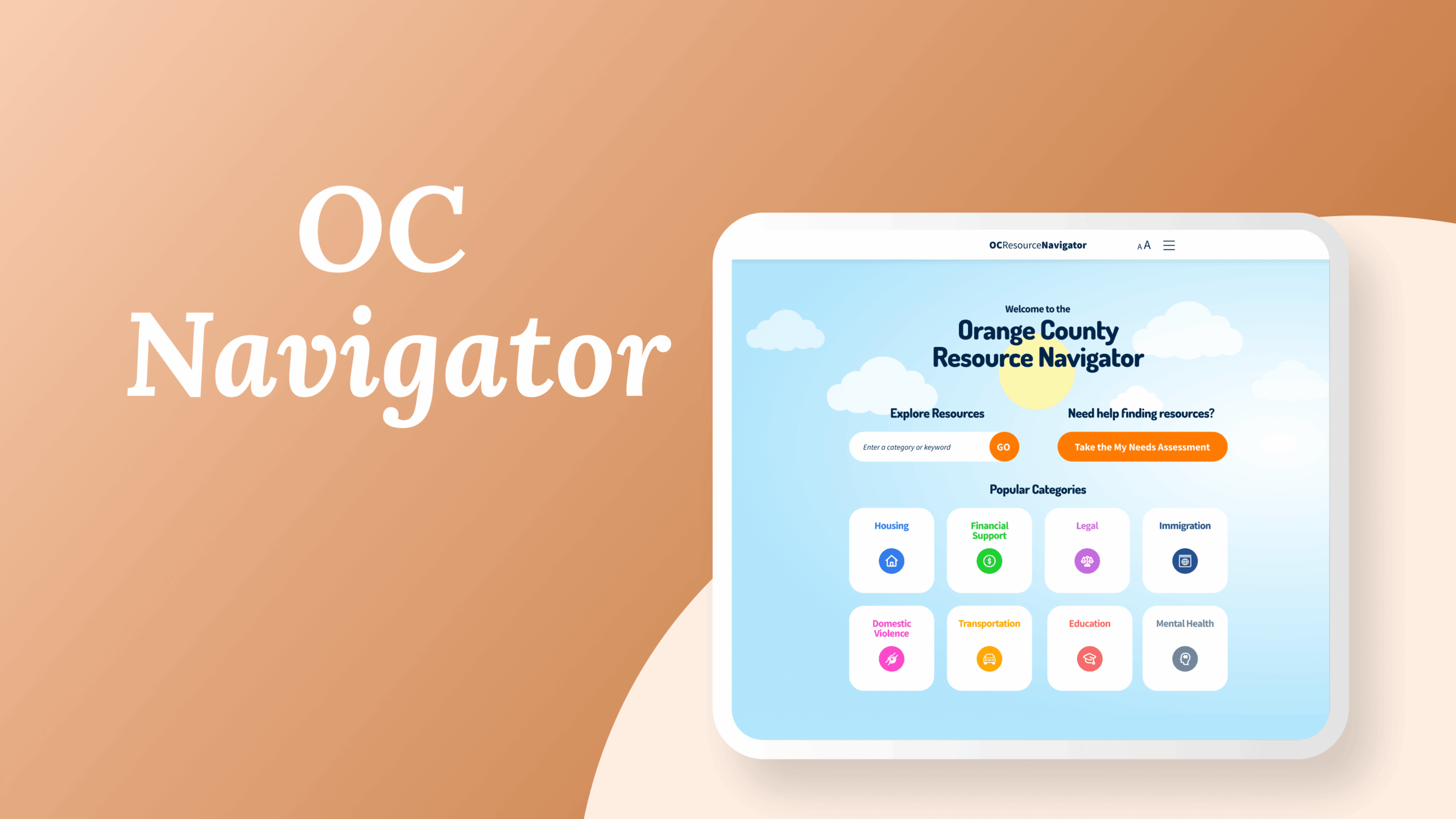
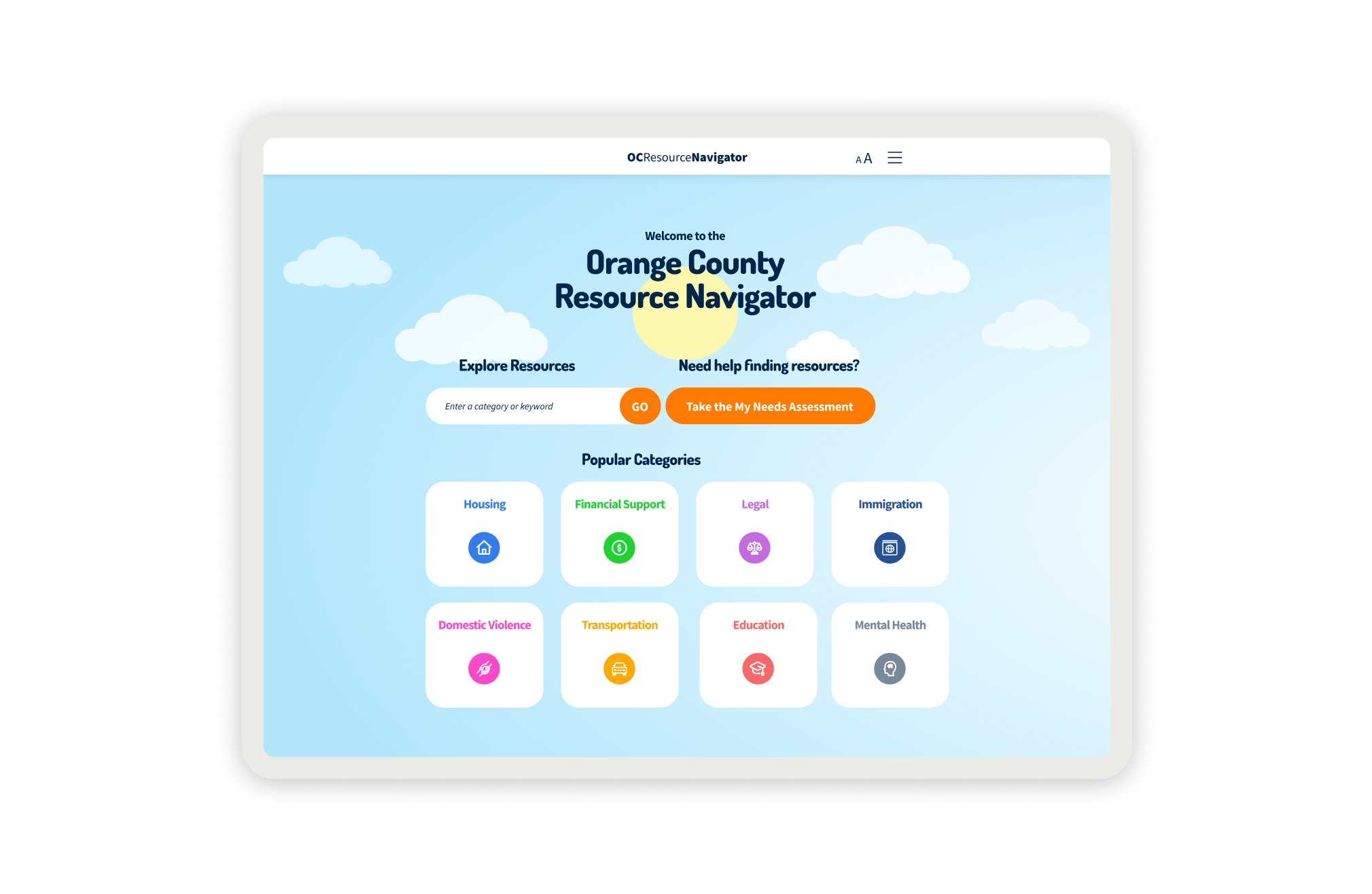
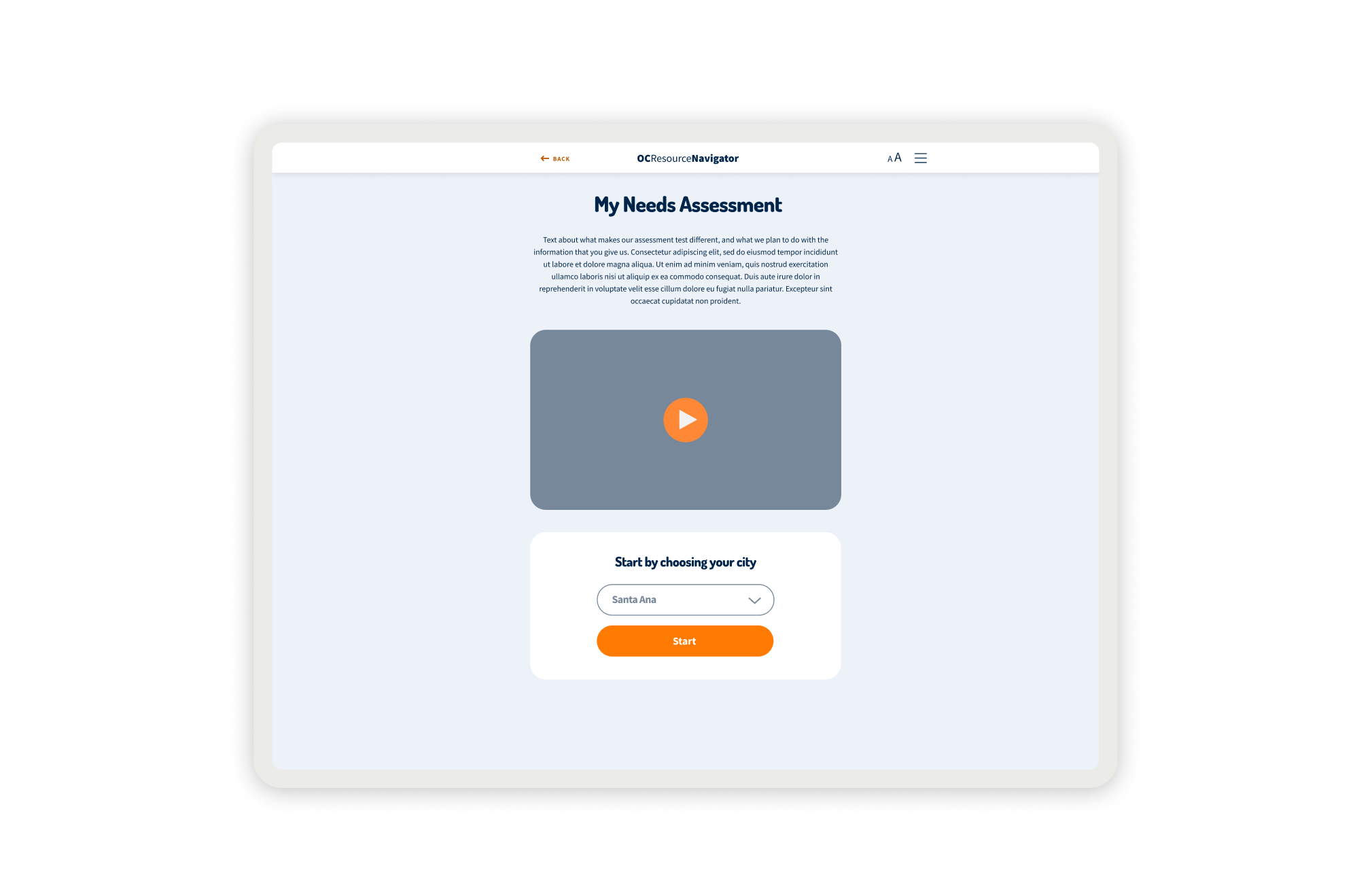
OC Navigator Demo
Shows how OC Navigator streamlines complex resource navigation into clear, personalized pathways for residents.
Design Interventions
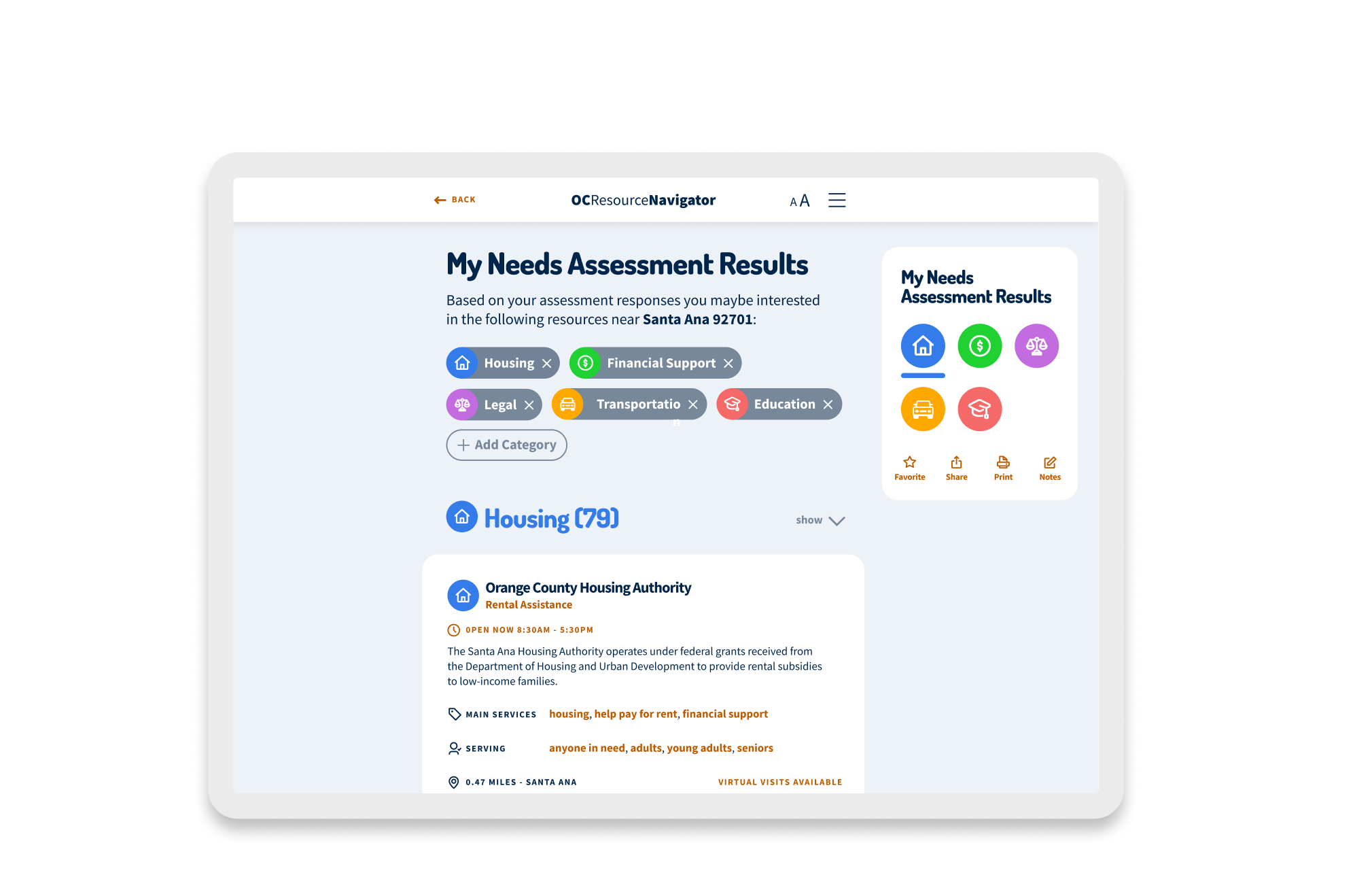
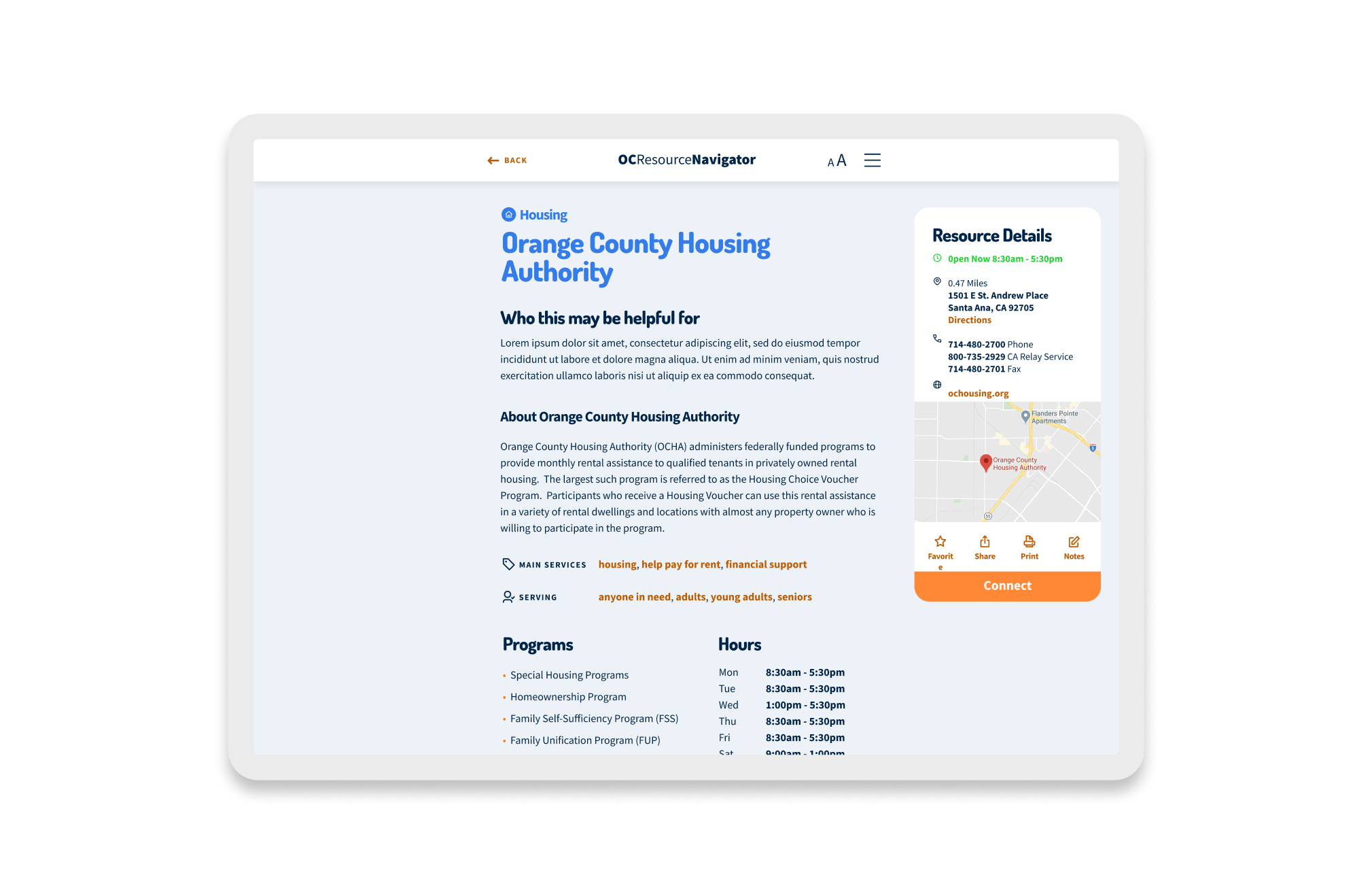
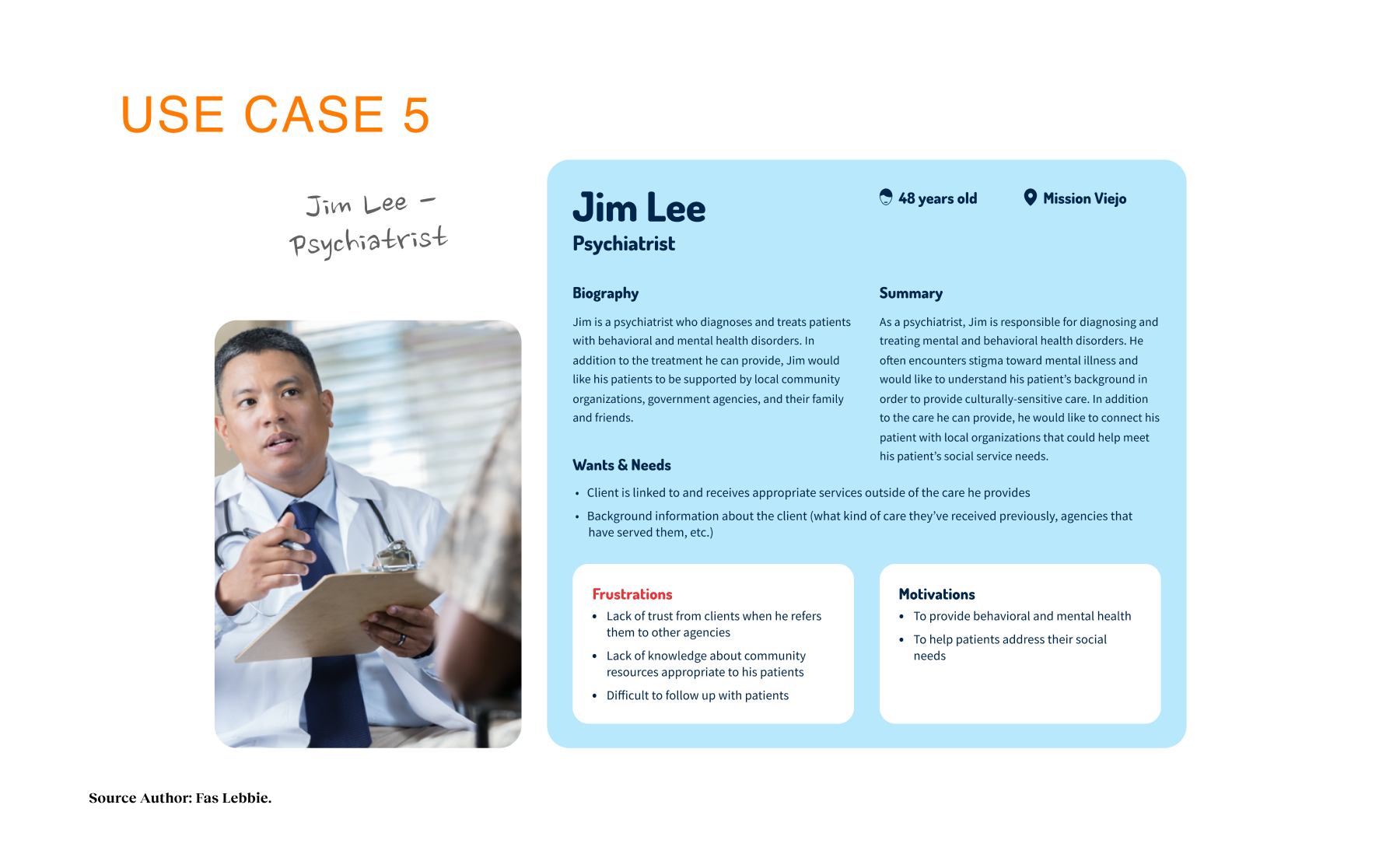
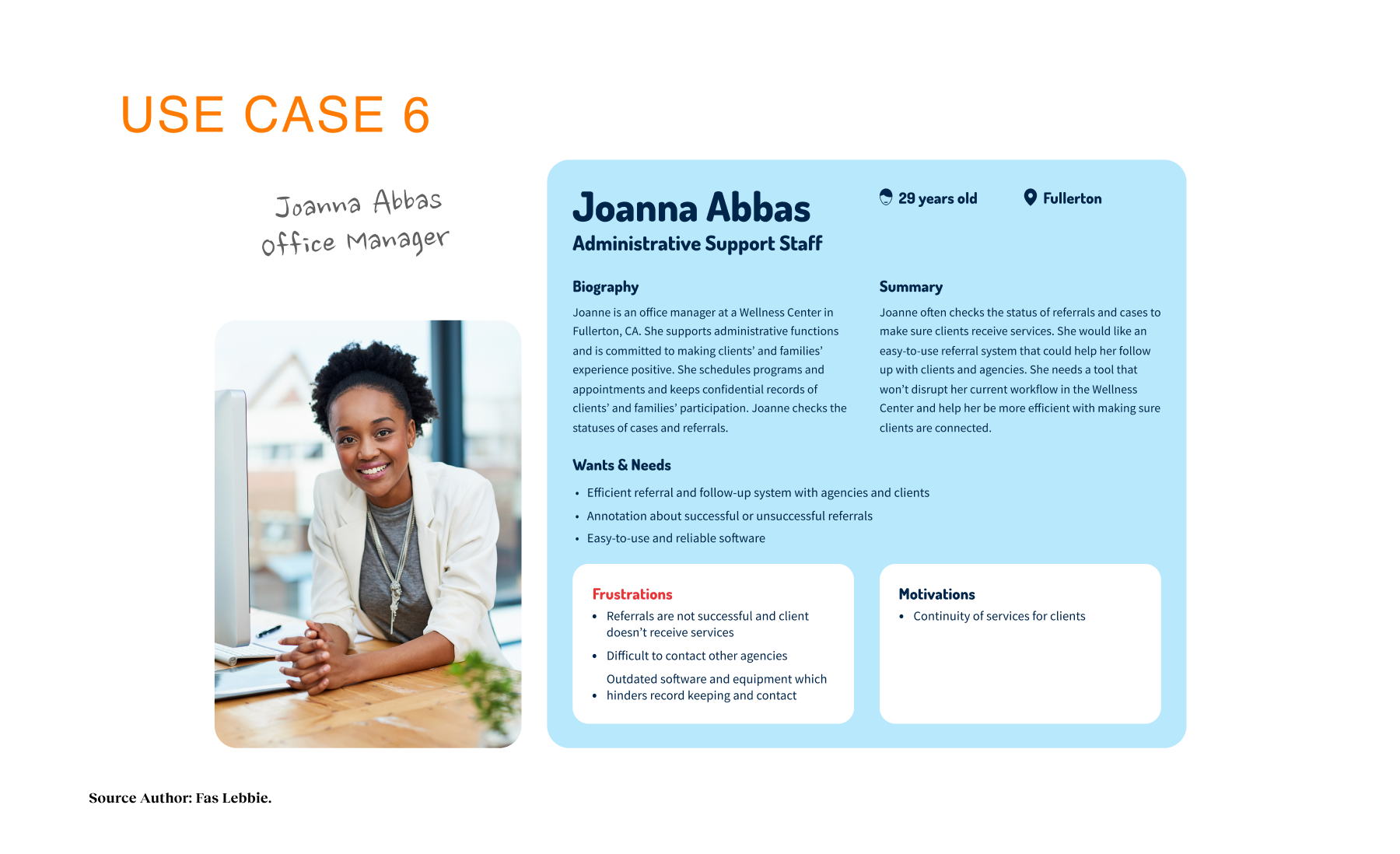
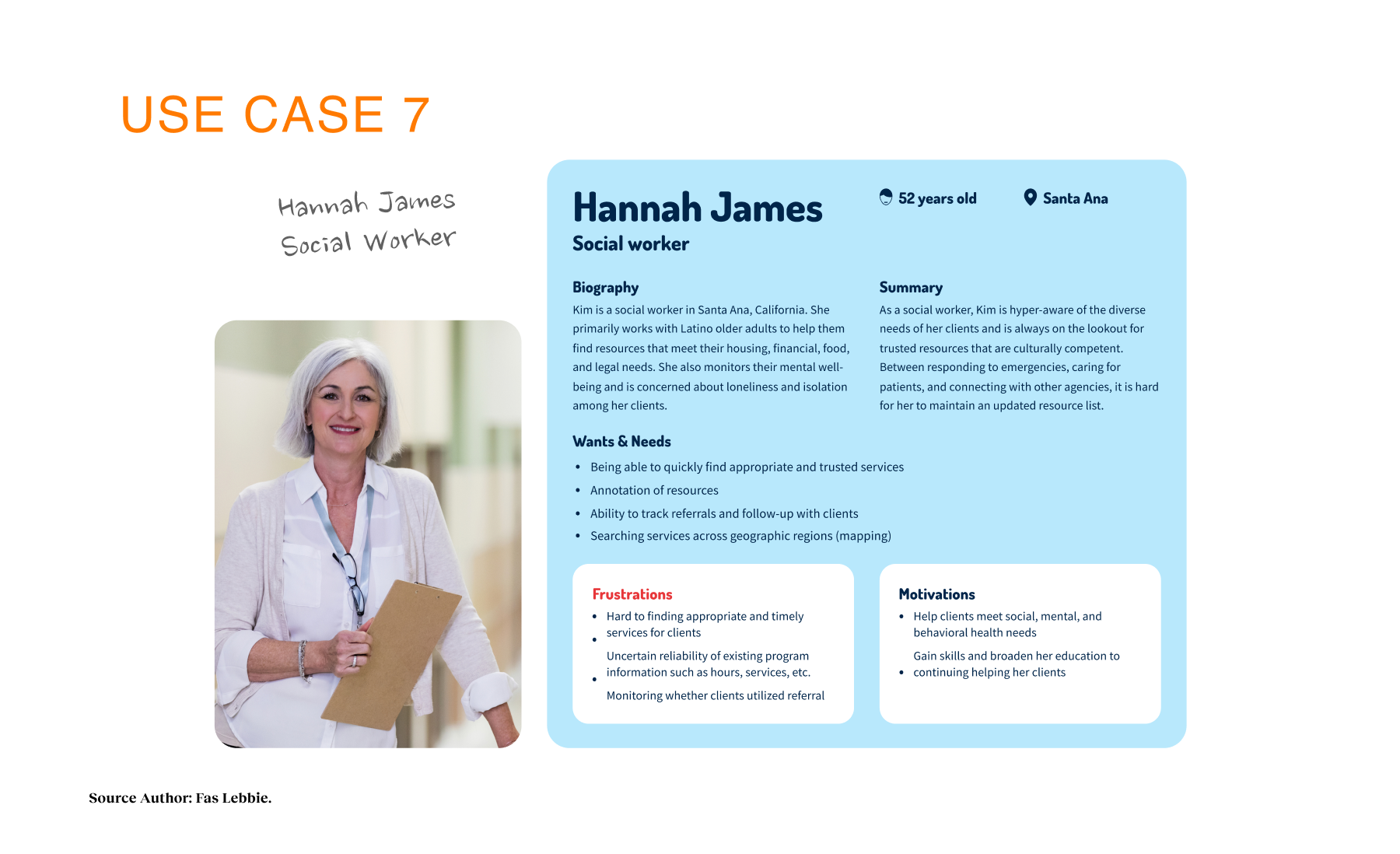
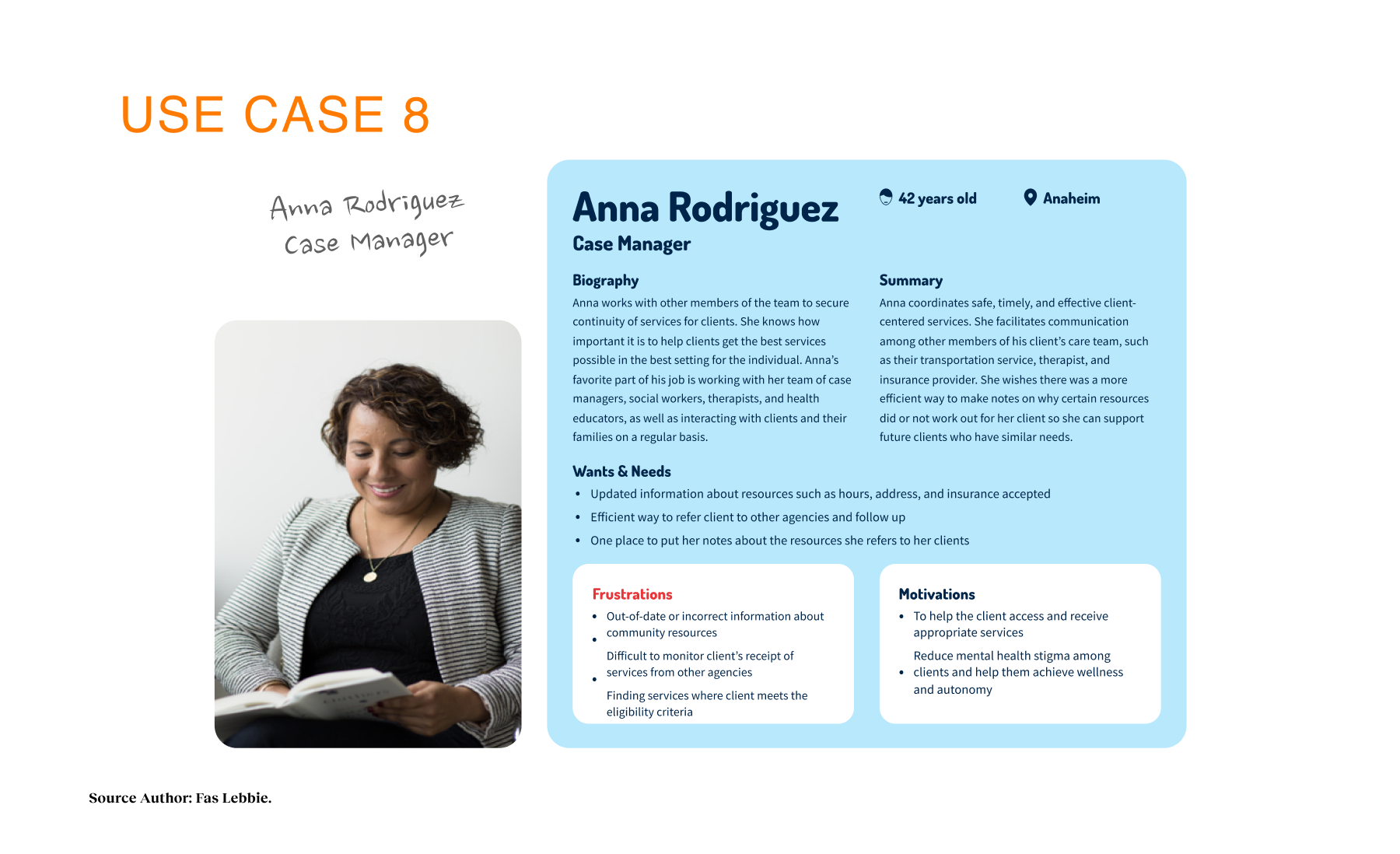
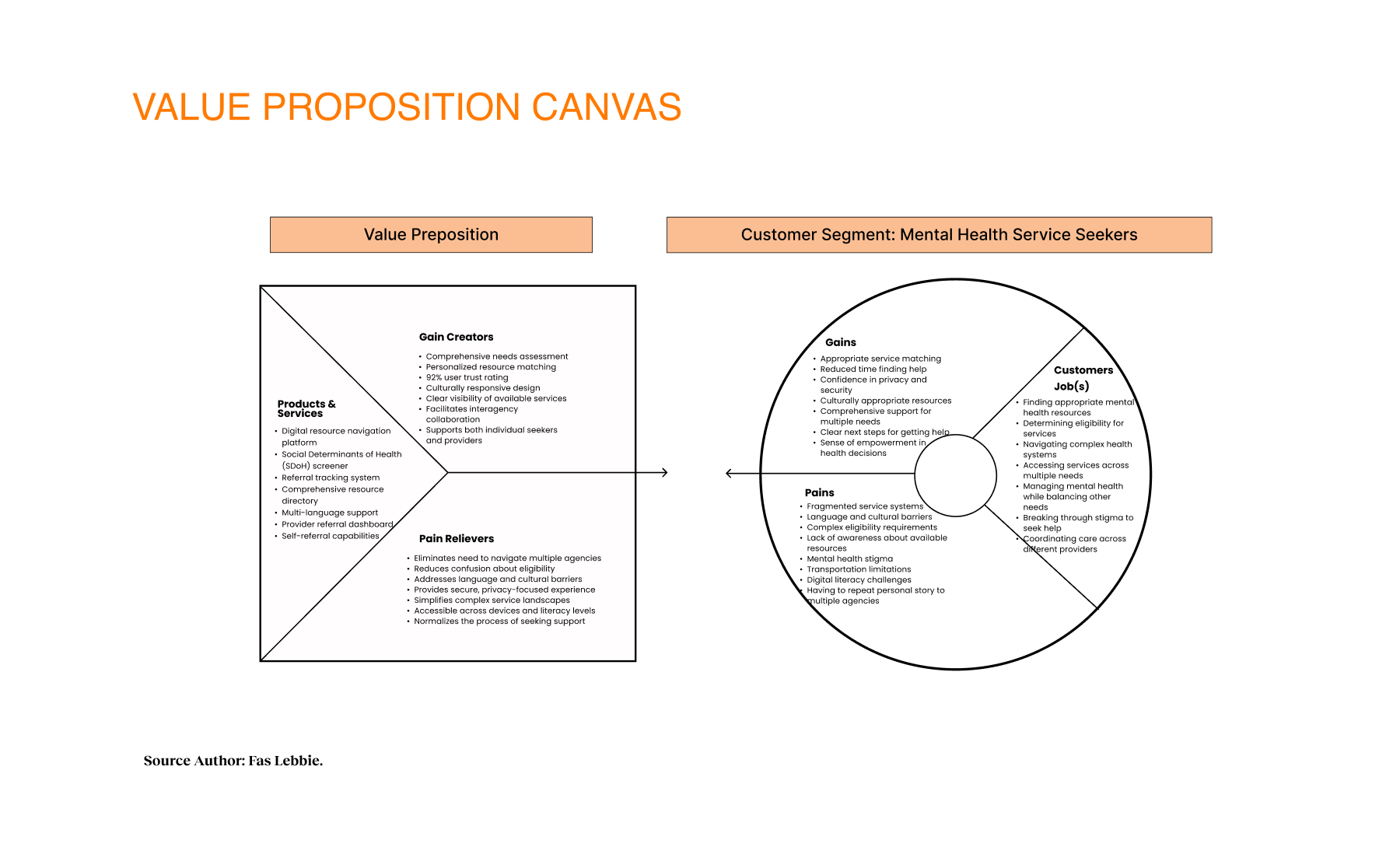
The design intervention targets individuals seeking mental health services and providers making referrals who struggle with fragmented resource navigation. The Navigator enables users to complete a Social Determinants of Health (SDoH) screener, matches their needs with appropriate resources, facilitates self-referrals or provider referrals, and allows users to track their referral progress. The core intervention was the creation of a dual-sided digital ecosystem: a “warm,” accessible front door for residents and a high-velocity command center for providers. We realized early on that a static directory would not solve the fragmentation crisis. Instead, we built an intelligent triage engine that acts as a connective tissue between the two groups.

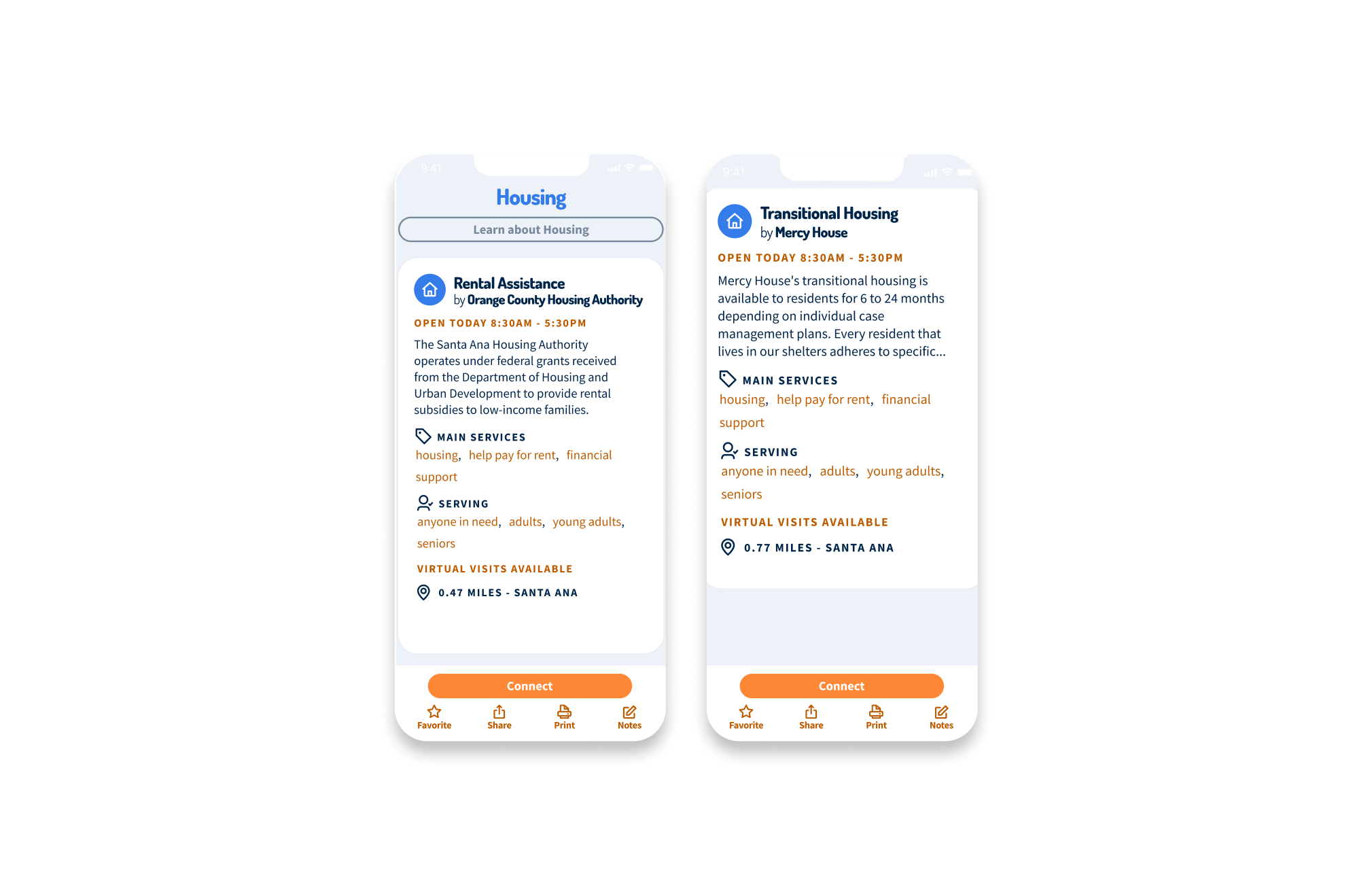
Individual
Social Worker

Office Admin

Service provider


Research Outputs
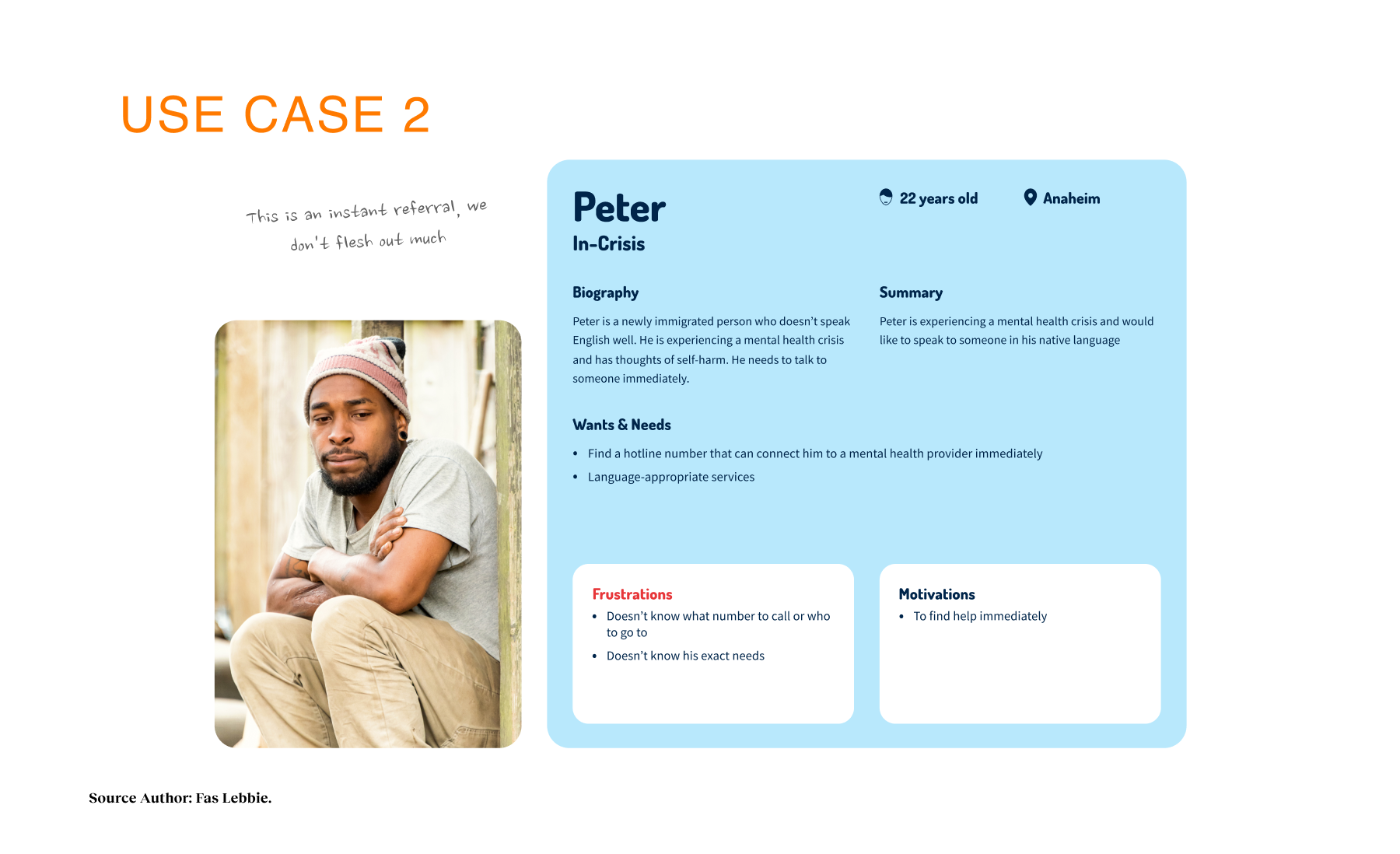
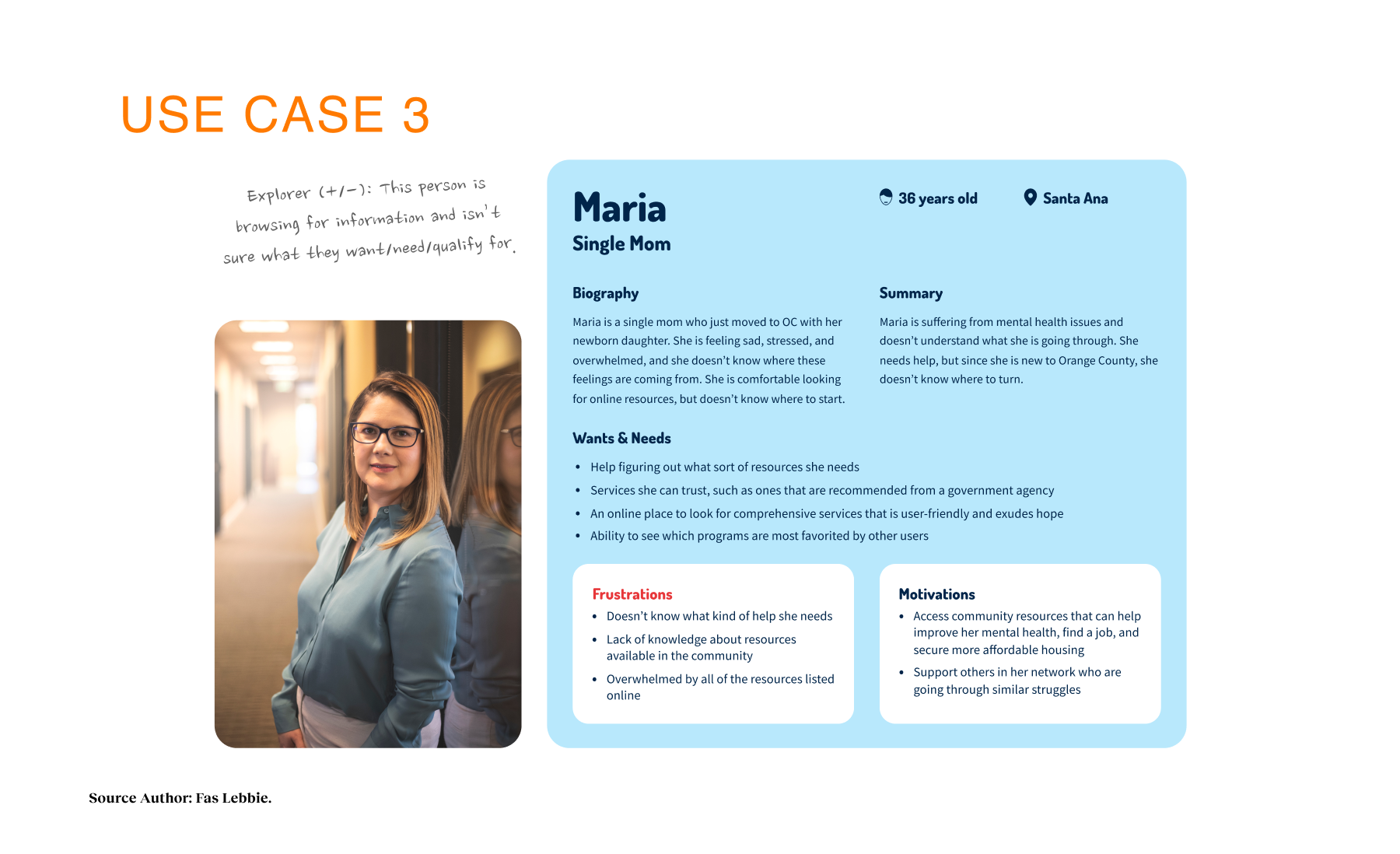
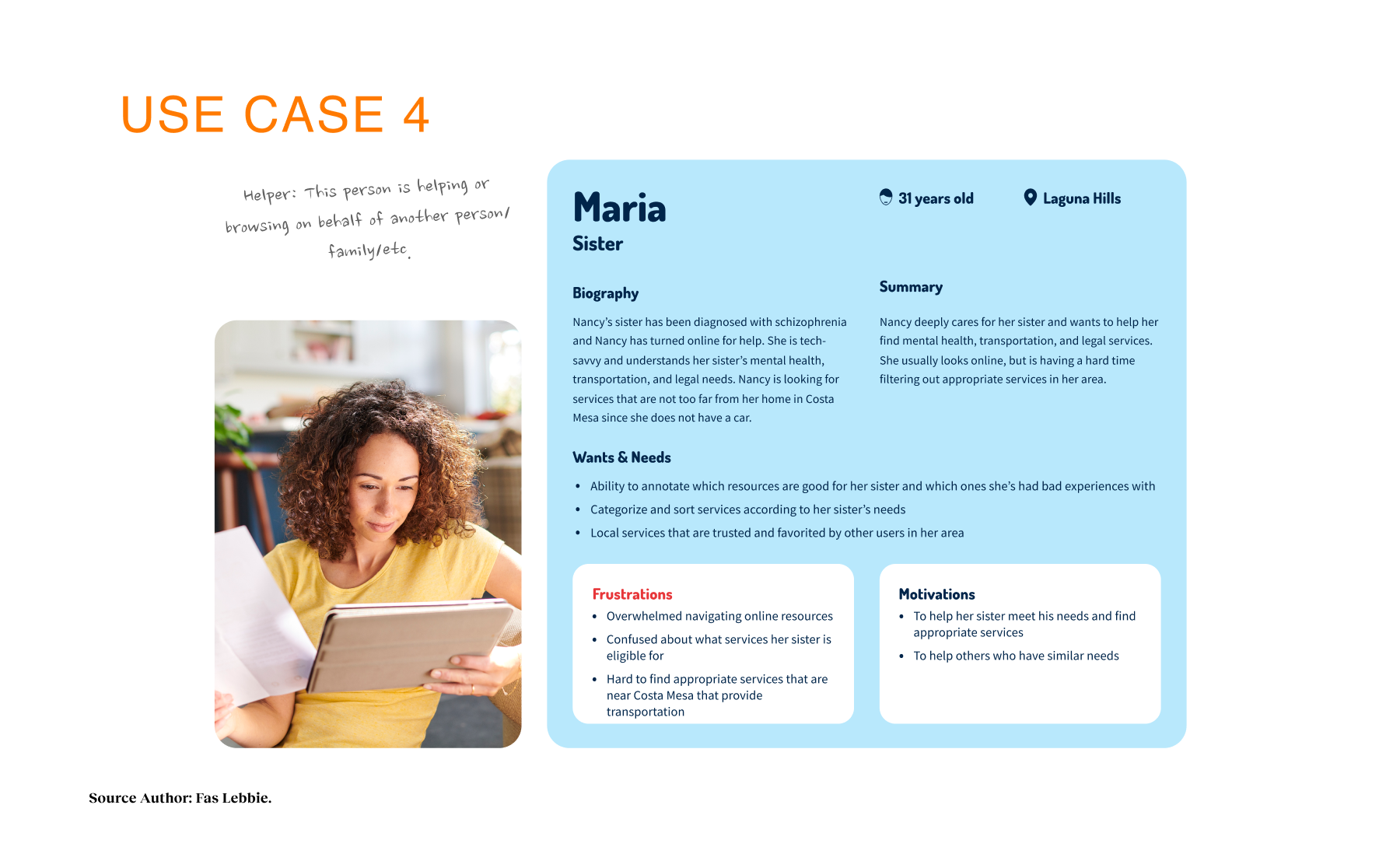
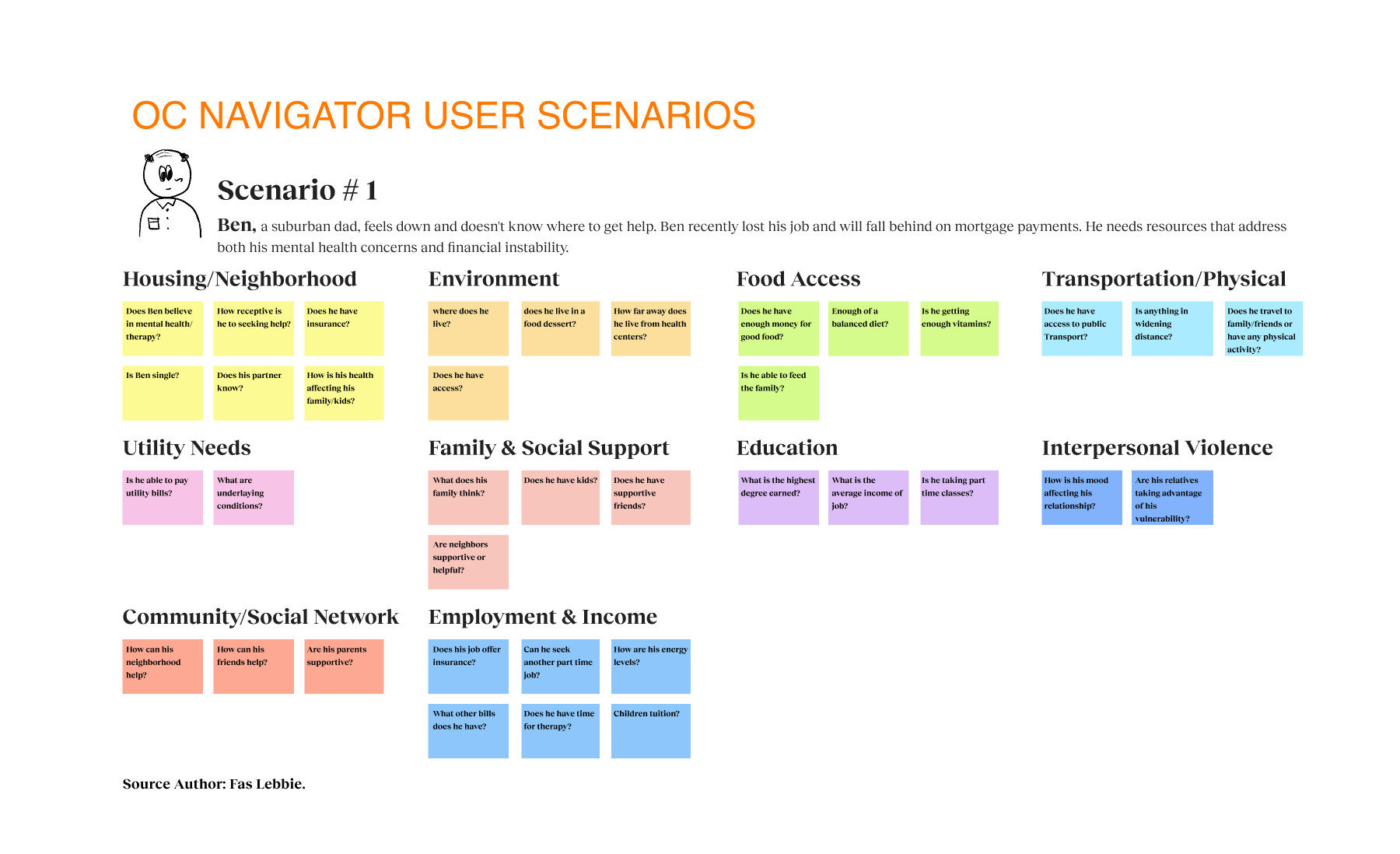
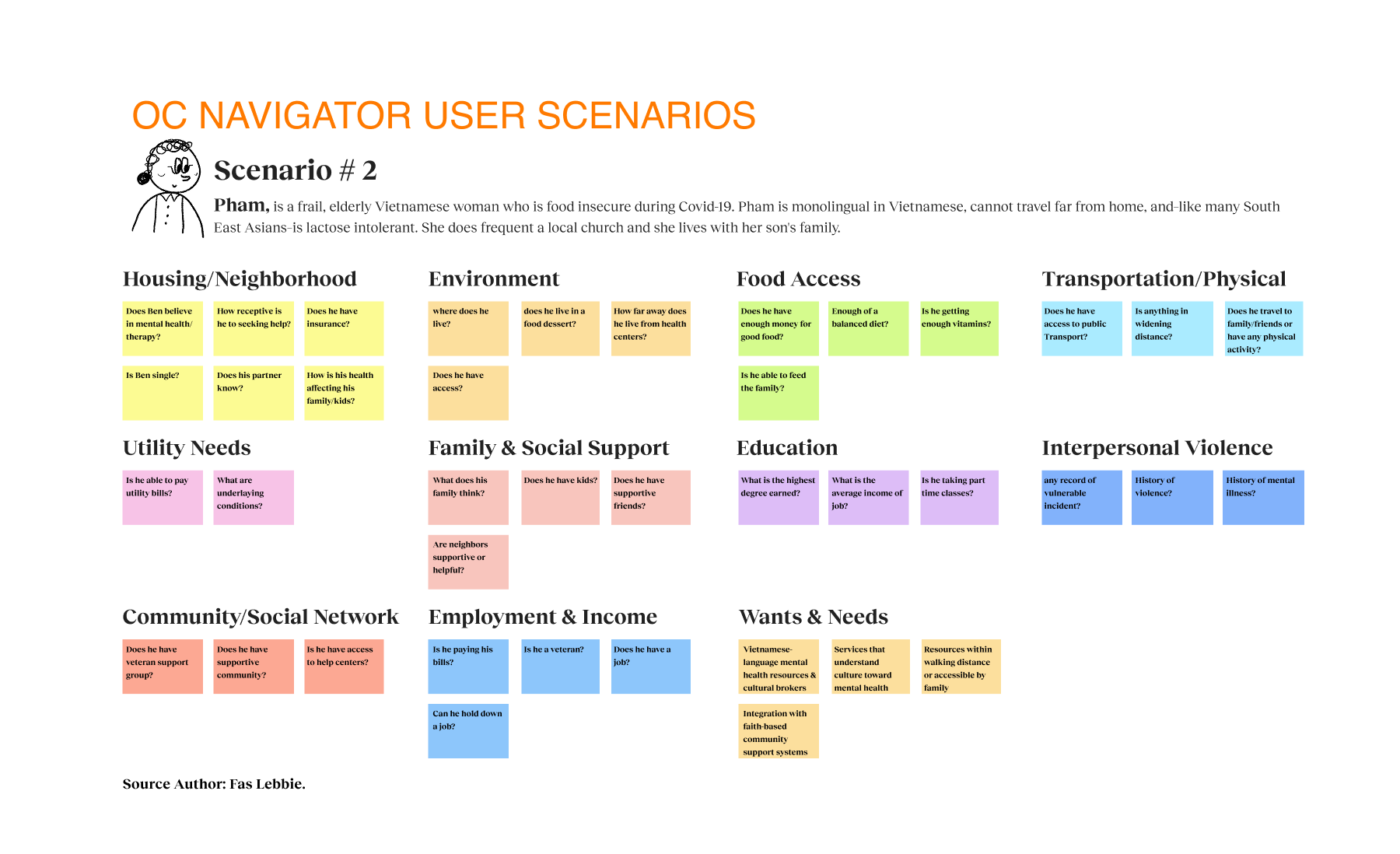
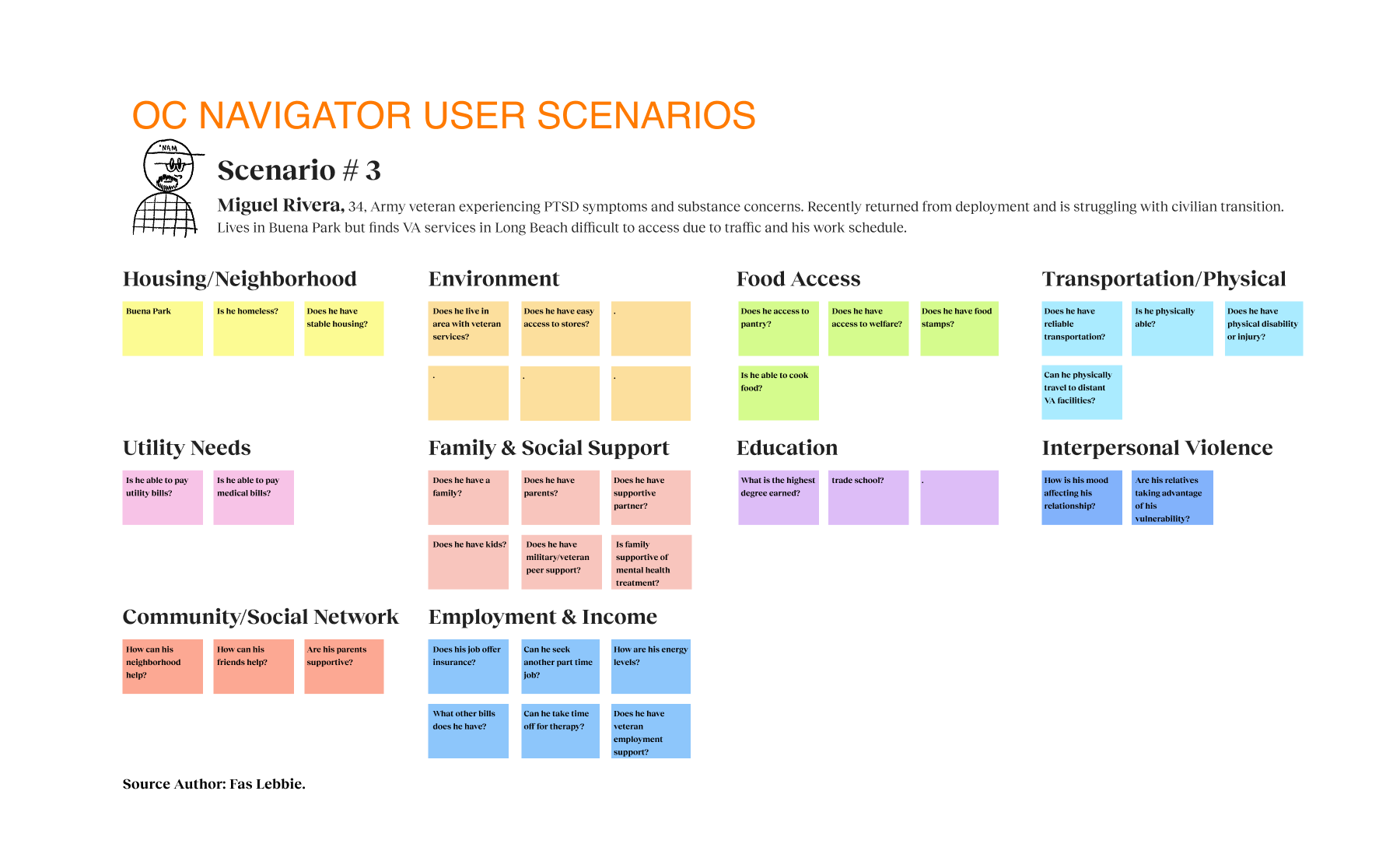
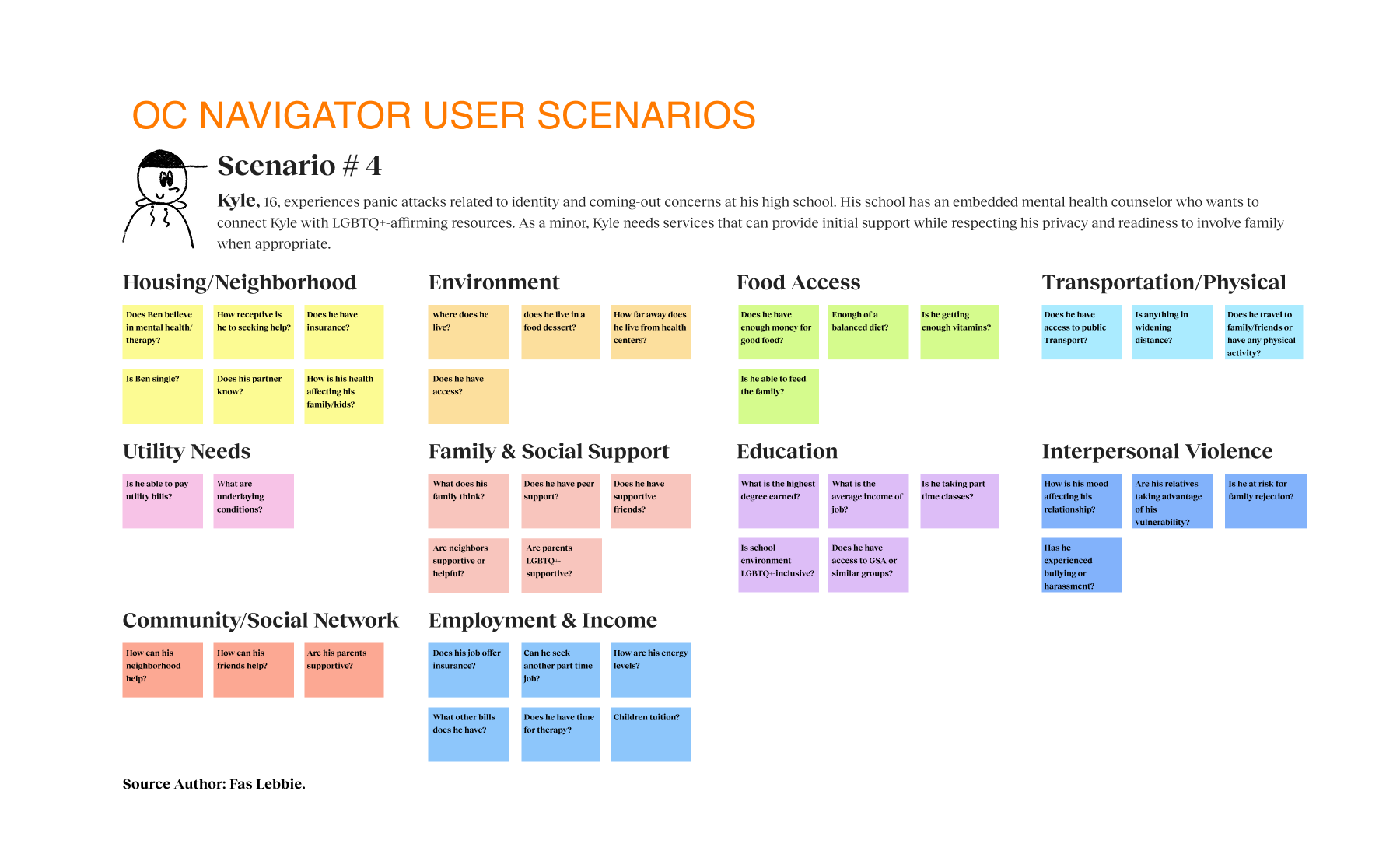
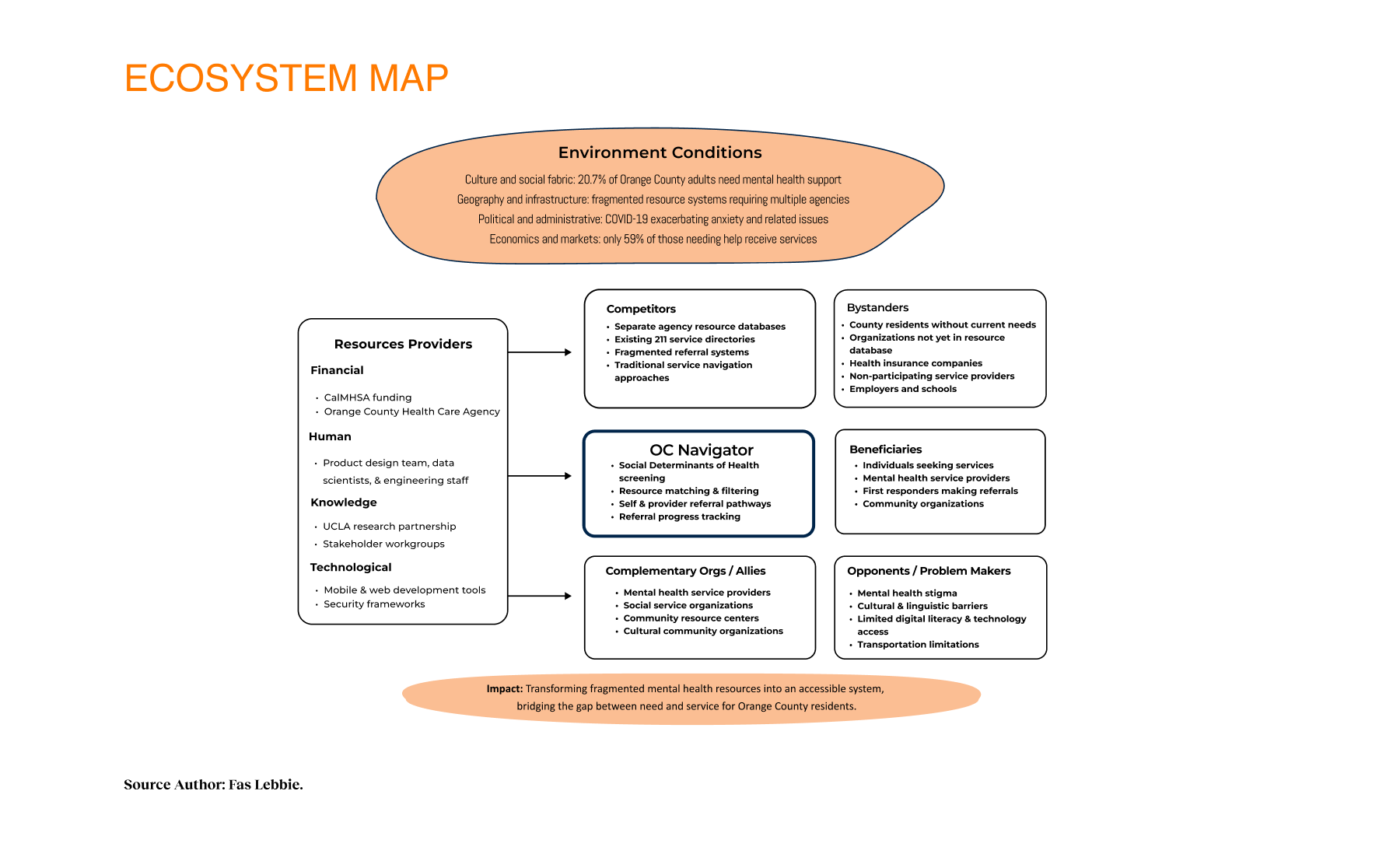
Participatory workshops shaped both the technology design and the values behind it, which emphasize transparency, partnership, and capacity building. We used Journey maps as the key driver of design decisions. Additionally, personas and lived-experience scenarios (e.g., veterans, immigrants, caregivers, youth, and the elderly) revealed the nuanced contexts shaping help-seeking behaviour. Building an extensive system map clarified the interplay of providers, competitors, allies, and barriers such as stigma and transportation.

Reduction In Crisis-Response Times
Reduced crisis-response times by 47%, enabling faster interventions for vulnerable users.
Increase In Referral Completion
Improved referrals by 35%, enhancing service follow-through and user outcomes.
Orange County Adults Needing Support
Represents over 650K residents requiring mental health services, demonstrating the massive scale of need addressed by the platform.
Reflections & Impact
Within the alpha phase, providers described how the tool supported clients in crisis, individuals found previously unknown services, and community organizations saw increased appropriate referrals. The initial resource categories expanded essential areas: housing, financial support, mental wellness, and food security. The design intervention focuses on a person’s whole journey rather than isolated touchpoints. This new system reflects communities’ wisdom, integrates local systems and partners, and uses participatory development. These principles yielded a platform addressing practical needs and emotional barriers to seeking help, normalizing the process of seeking support. By incorporating the social determinants of health screening into navigation, we’re shifting how the mental health system considers comprehensive care. The platform provides a foundation for greater interagency collaboration and data-informed resource allocation as part of the Behavioral Health System Transformation initiative, which addresses a universal need for coordinated mental health resource navigation that transcends geographic boundaries. As adoption increases across Orange County, the project can transform fragmented services into a coordinated system of care.
Next Steps
- Expand Provider Dashboard with referral tracking and outcome measurement to improve accountability and service follow-through.
- Integrate with Health Records for seamless coordination between county systems and providers.
- Develop Culturally Responsive Access by adding a Spanish-language interface and tailored resource categories.
- Create a Mobile App for Accessibility optimized for offline use in low-connectivity areas.