Overview
This initiative unified Orange County’s behavioral health landscape, transforming a disconnected network of services into a single, integrated digital crisis management platform. By modernizing the $18M initiative’s infrastructure, we didn’t just update software; we closed the system gaps that were leaving vulnerable people in the cracks. Orange County’s behavioral health system serves over 650,000 residents and relies on a complex web of partners, including CalMHSA, NAMI, and the Crisis Assessment Team. However, the infrastructure supporting these critical services was fracturing under the weight of outdated technology and silenced communication channels. For years, responders were forced to navigate a fragmented ecosystem where three distinct services operated on separate, antiquated platforms. This lack of integration meant that critical data and, more importantly, people in crisis, could easily get lost during handoffs between agencies. The system was rich in resources but poor in connectivity, leading to inefficient budget allocation and frustrating delays for those seeking help. I led research and design, partnering with Chorus Innovations and county stakeholders. We created a unified platform that integrates workflows, ensures privacy compliance, and connects residents to trained Navigators 24/7, thereby accelerating access to care.
Research & Design
Mixed-methods research · Integrated platform design · Healthcare privacy compliance · Crisis workflow analysis Compliance: Accessibility (WCAG) · Healthcare privacy (HIPAA)
- Duration: 2022
- Partners: CalMHSA, OC Links, NAMI, Crisis, Chorus Innovations
- Team: Fas Lebbie, Parker Gibbons, Sage Bennett
Confidentiality: Some details have been altered to safeguard sensitive information, while highlighting my design approach and insights to maintain confidentiality.
My Role
I directed the experience design for core call management and chat systems, developed an integrated resource directory and referral workflow, conducted qualitative and quantitative research with crisis responders and clients, and designed web app interfaces that effectively balanced clinical needs with user experience best practices.
WHAT I BROUGHT
I steered the strategic vision for an integrated platform that had to interface with complex healthcare privacy and accessibility compliance standards. This required aligning diverse stakeholders around a shared "Single Point Access" framework, ensuring we solved for systemic cohesion.
I conducted mixed-methods research strategy, utilizing contextual inquiry and crisis workflow analysis to expose hidden inefficiencies. My focus was on moving beyond surface-level user complaints to uncover the structural "workarounds" responders used, such as manual notes and side conversations, that generated the evidence needed to improve legacy systems.
I architected the core flows for a unified ecosystem, designing a system that seamlessly handles complex permission structures and secure inter-agency handoffs. I focused on creating intuitive navigation and clear visual hierarchies that support rapid decision-making in high-stress, high-stakes environments.
I facilitated deep collaboration between OC Links, the Crisis Team, and NAMI/WarmLine, helping these distinct agencies agree on standardized workflows. Through workgroup sessions, I helped operational partners see the value in shifting from isolated databases to a shared, transparent information architecture.
Problem Context
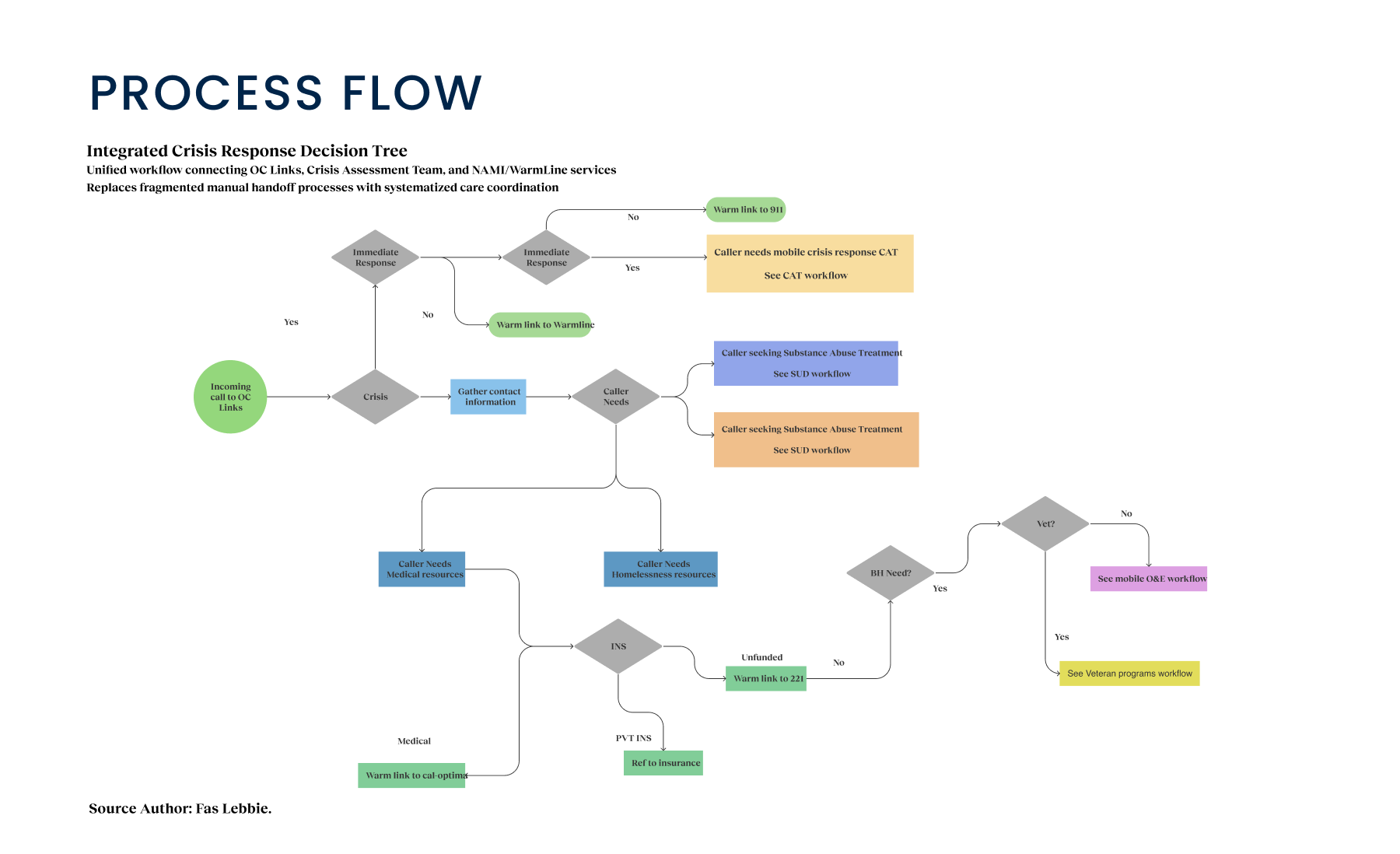
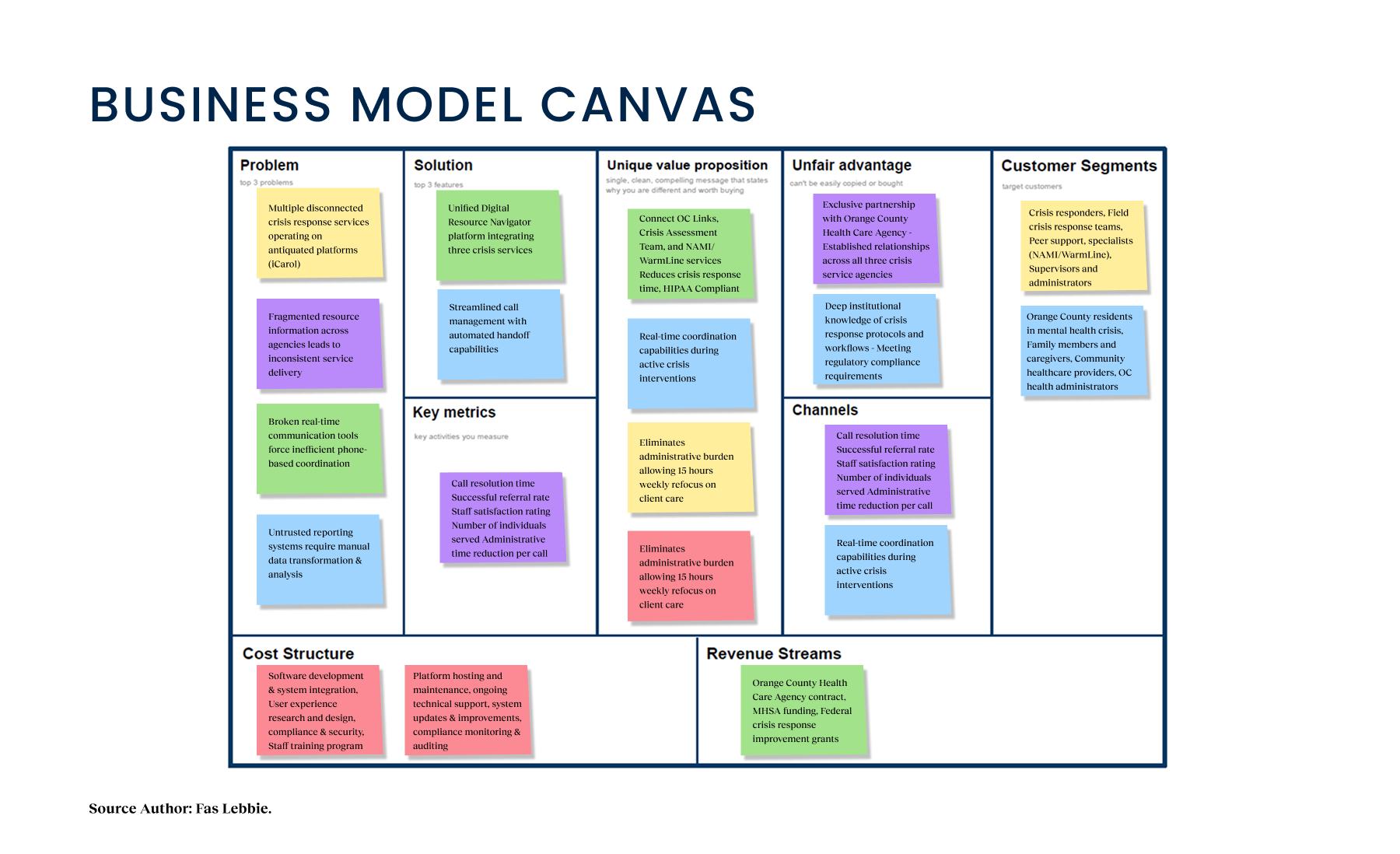
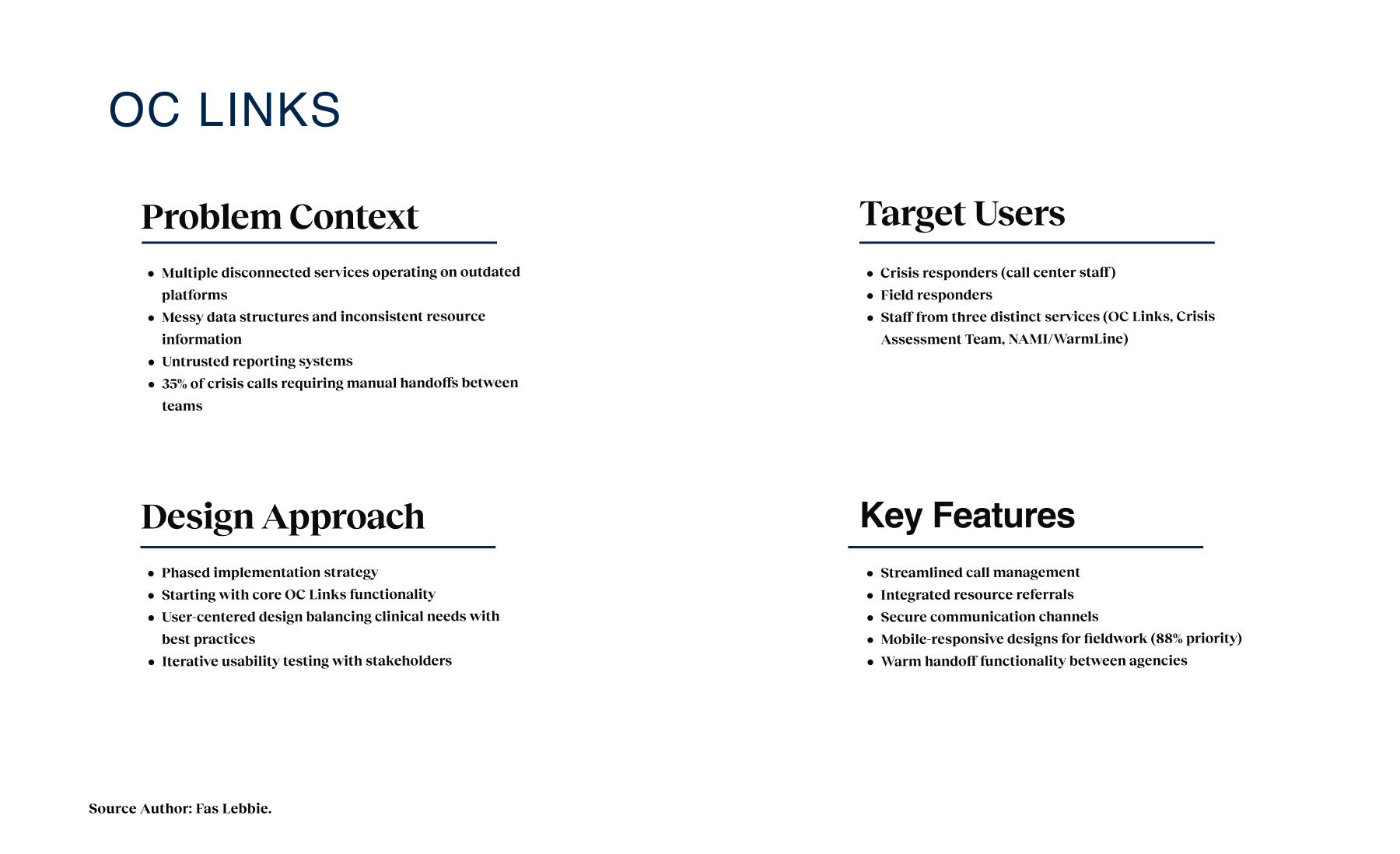
The mental health crisis response system in Orange County consisted of multiple disconnected services on outdated platforms. The system was a patchwork of disconnected services running on iCarol, an outdated software platform notoriously difficult to navigate. While the staff’s intentions were heroic, their tools actively worked against them. We found that three interconnected services, OC Links, the Crisis Assessment Team, and the NAMI WarmLine, were effectively functioning as islands. Data structures were messy and inconsistent, making it nearly impossible to track a caller’s journey across different agencies. If a resident needed to be transferred from a warm line to a crisis team, the information transfer was often manual and prone to error. The friction wasn’t just administrative; it was dangerous. Critical gaps emerged: vulnerable populations needed immediate intervention, but the system’s inability to facilitate real-time communication or trustworthy reporting led to delays. Responders were spending valuable minutes wrestling with software rather than supporting clients. The fragmentation led to inefficient resource allocation and, most critically, missed opportunities for intervention in a field where timing is everything.
My Approach
I realized early on that we weren’t just fixing software; we were repairing trust in a fractured system. The legacy infrastructure forced responders to choose between accurate data entry and clinical empathy, creating a massive administrative burden. My strategy centered on leveraging deep research to architect a unified ecosystem focused entirely on the human in crisis, designing not just for efficiency, but for the moment of connection.
Design Process
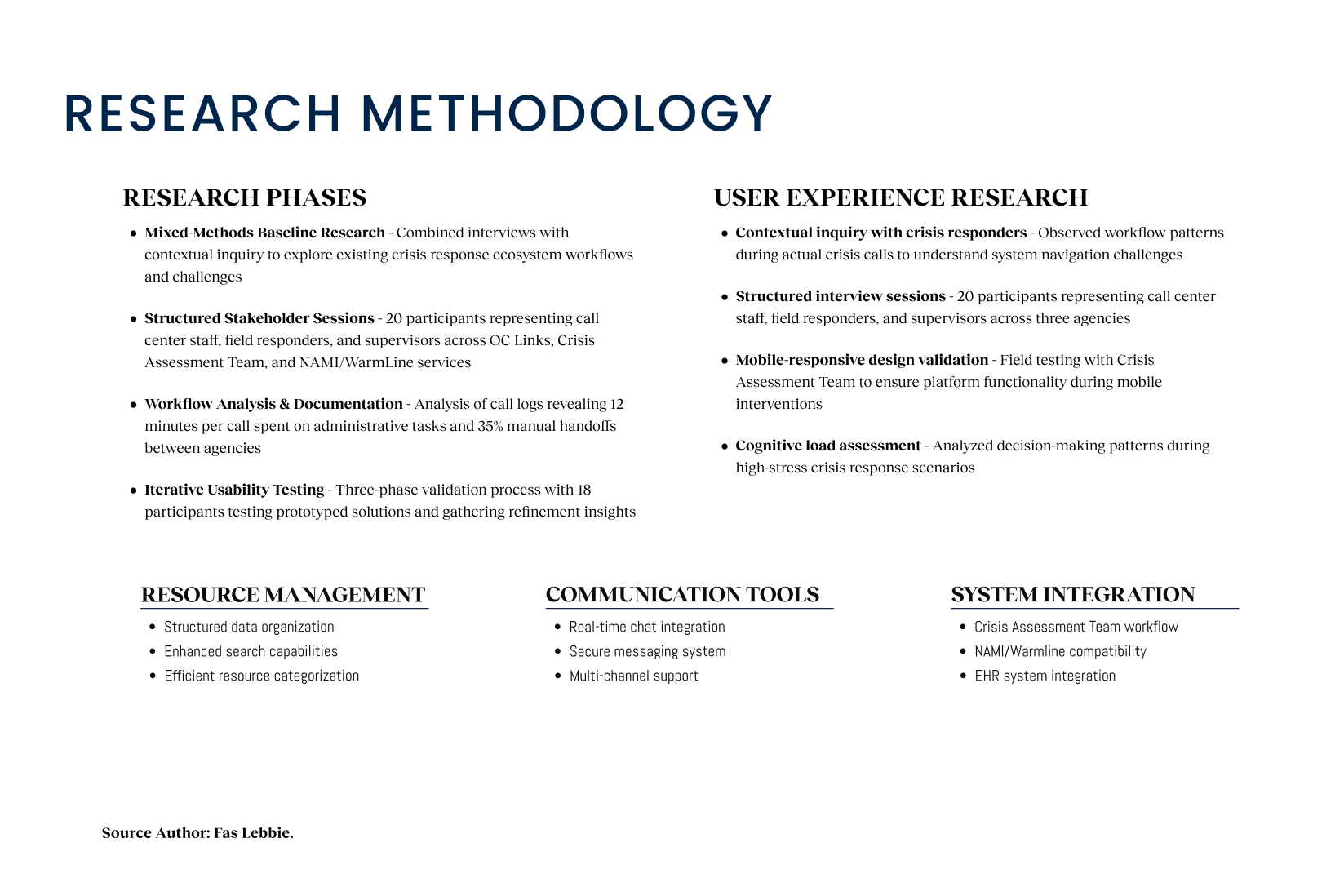
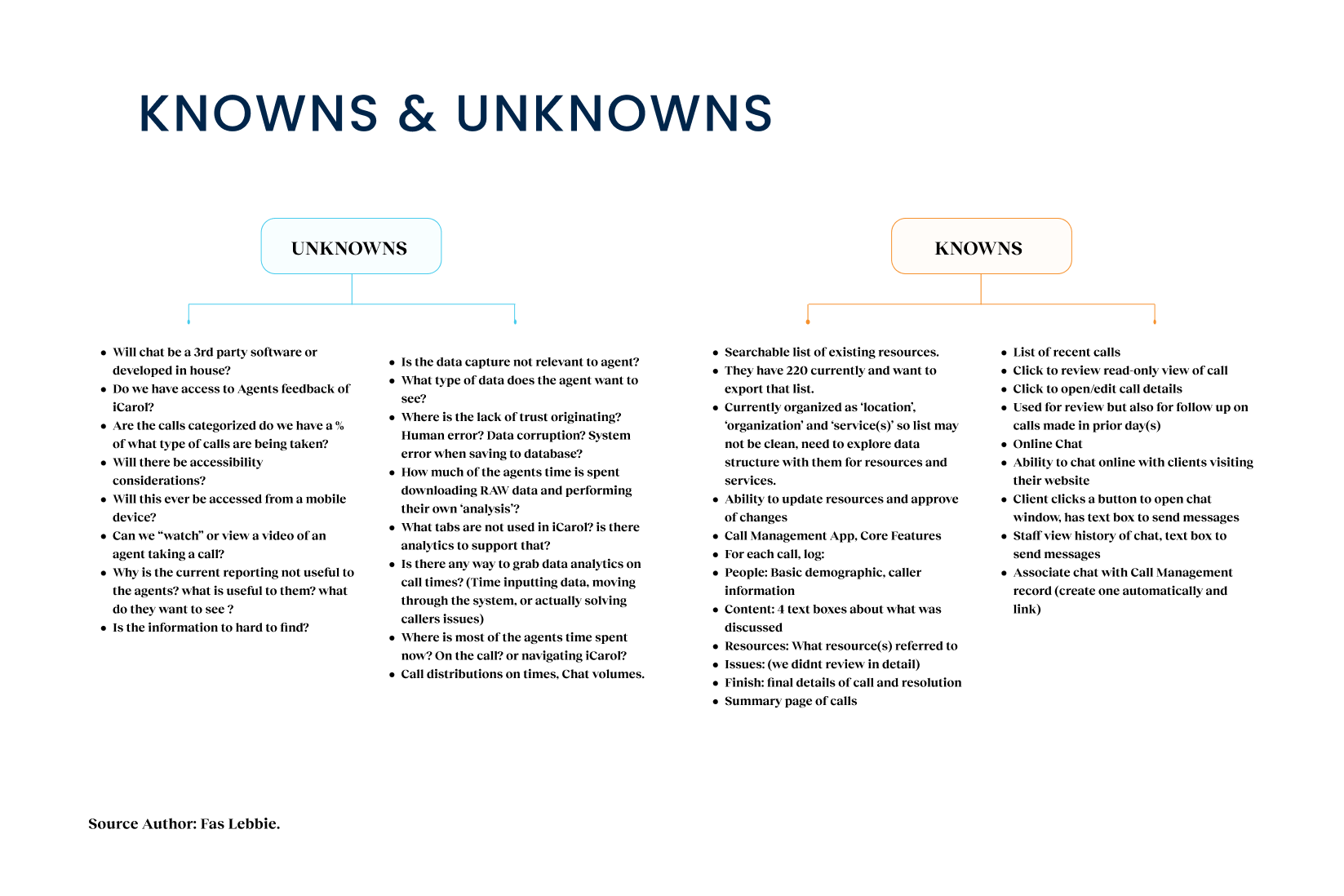
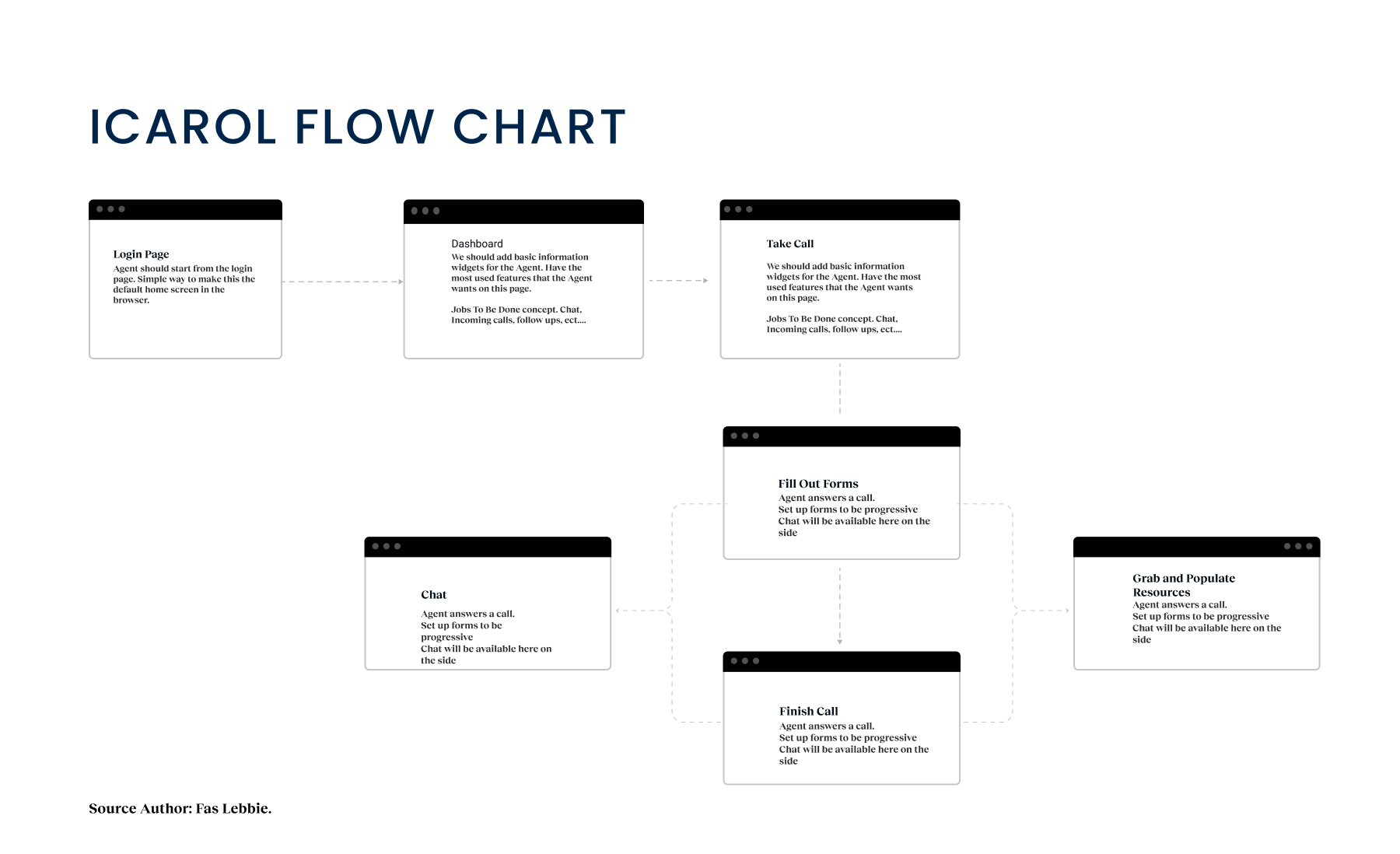
Starting this project felt like stepping into a time capsule of legacy IT. The ecosystem was defined by fragmentation; we had three distinct services operating on separate platforms despite serving overlapping populations. There was no “single source of truth.” Early observations signaled that crisis responders were using iCarol, an outdated system that lacked basic modern navigation patterns. Resource management data was unstructured, making it hard for a navigator to find or trust the availability of a clinic or shelter. Quantitatively, the baseline was inefficient. Call logs suggested that responders were spending roughly 12 minutes per call just on administrative tasks, typing, searching, and verifying, rather than direct support. Real-time communication tools like chat were either broken or missing entirely, forcing staff to rely on phone calls even when text might be safer or more discreet for the client. Reporting was a manual nightmare, requiring significant data transformation just to get a basic read on weekly performance.
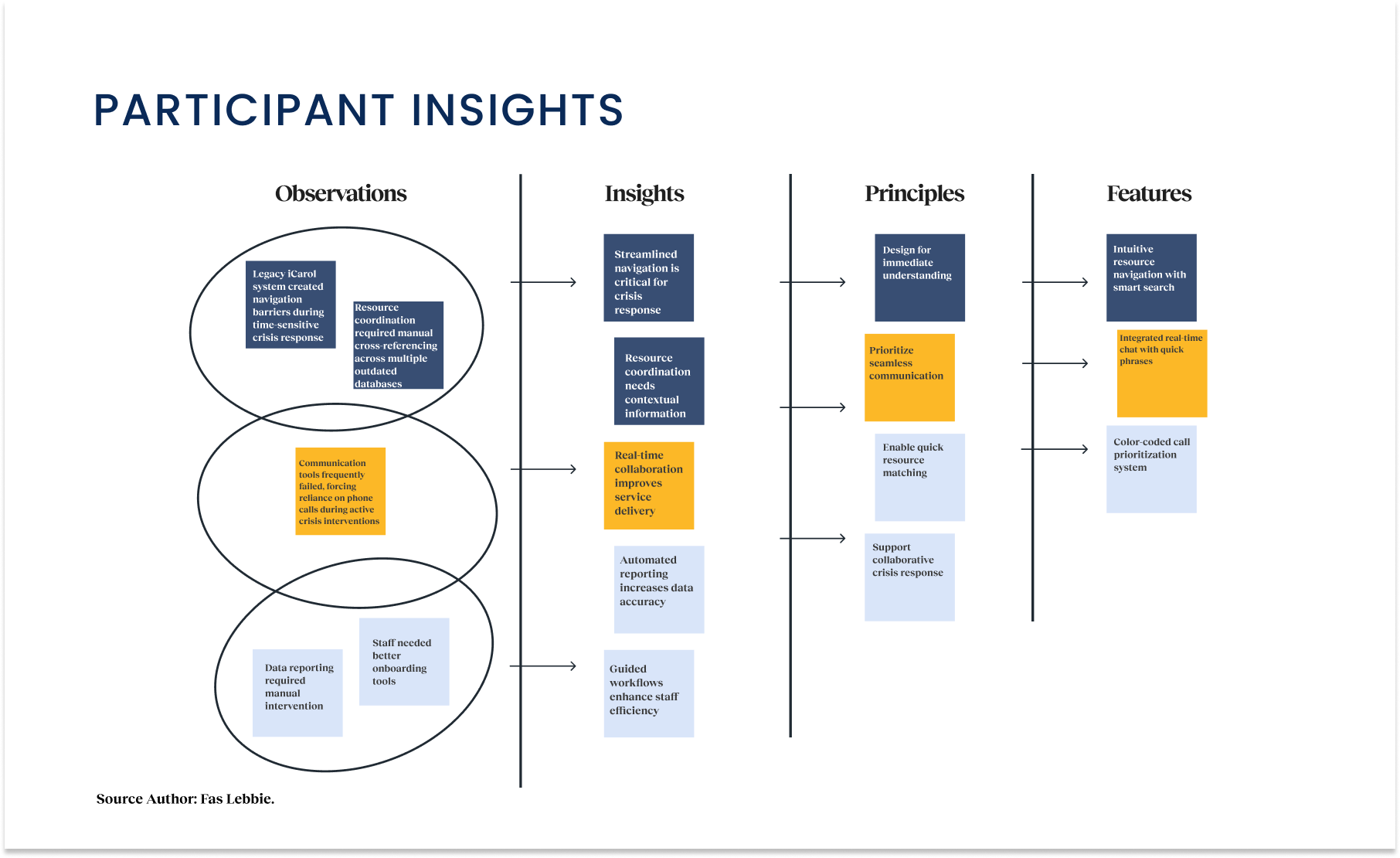
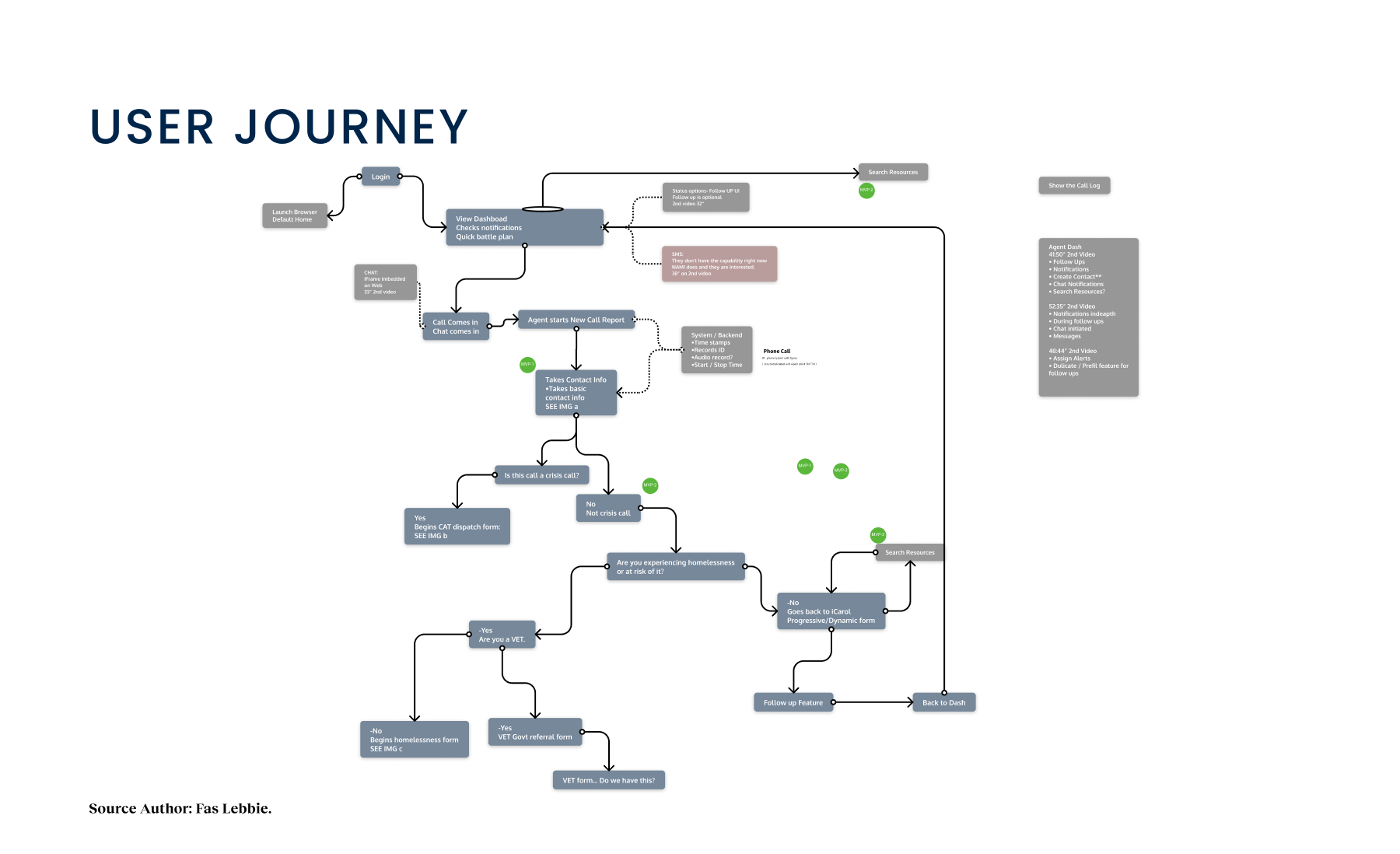
The system was fragmented, with three distinct services (OC Links, Crisis Assessment Team, and NAMI/WarmLine) operating on separate platforms despite serving overlapping populations. I led a mixed-methods research approach to understand the “why” behind the workflows. We combined stakeholder interviews with contextual inquiry, sitting alongside the people who answer the phones and manage the crises. I conducted structured sessions with 20 participants across the ecosystem, including call center staff and field responders. My objective was to map the full crisis response ecosystem, specifically looking for the “invisible work” the sticky notes, side conversations, and manual workarounds used to bridge gaps between software silos. We utilized Stakeholder Activity Mapping and Ecosystem Mapping to visualize these disconnects. This visual evidence was crucial. It allowed us to move the conversation from “we need a new platform” to “we need to fix the workflow.”
The research phase peeled back the layers of operational friction, revealing that the software wasn’t just working barely; it was costing the county significantly in lost time and potential outcomes.
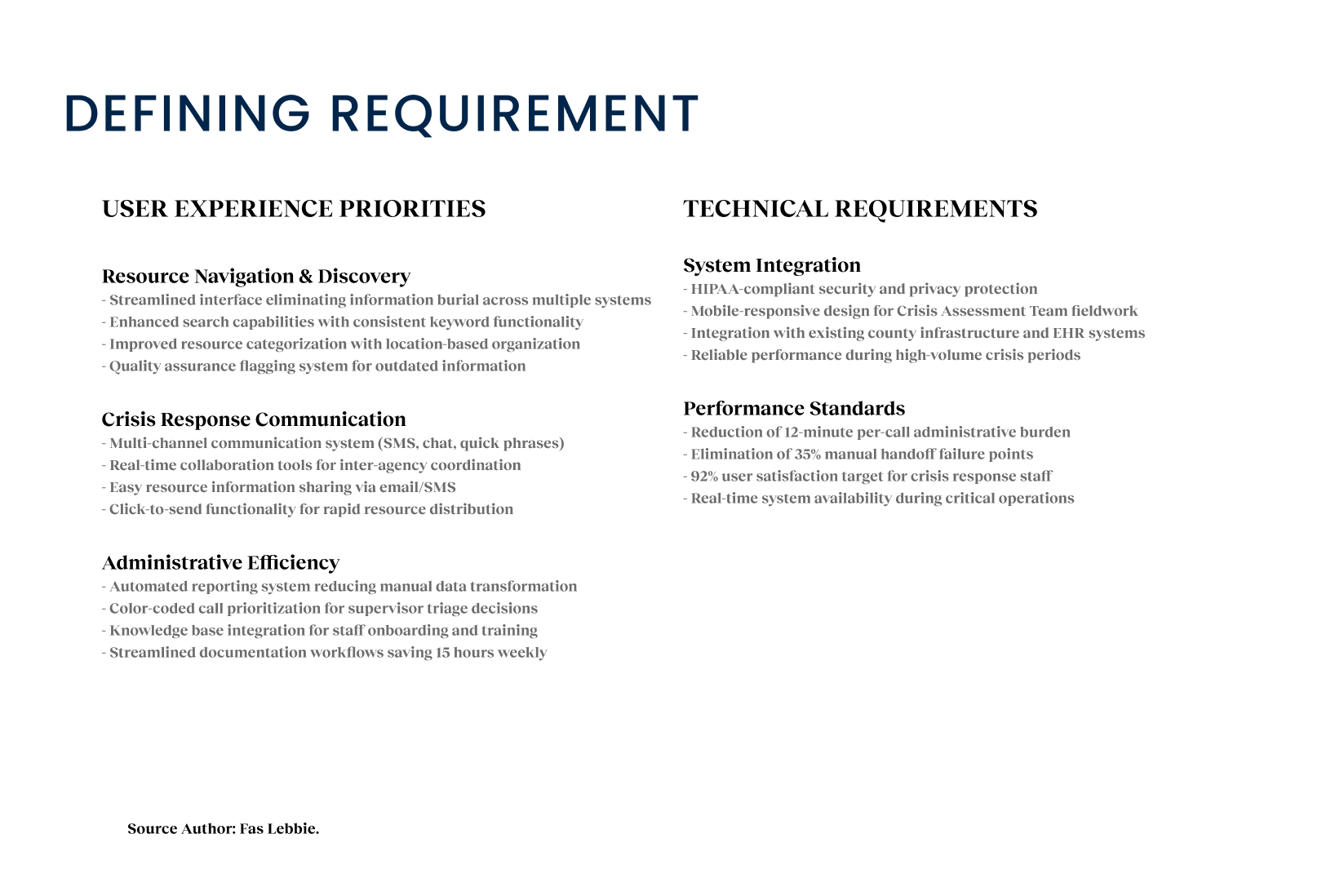
- We discovered that responders were spending 12 minutes per call on administrative tasks. This wasn’t just downtime; it totaled 15 hours per person per week. A time that could be automated. In a resource-limited public health setting, this was a massive, avoidable cost. For the Design Implication, we needed to automate intake fields and unify data entry to reclaim this time for patient care.
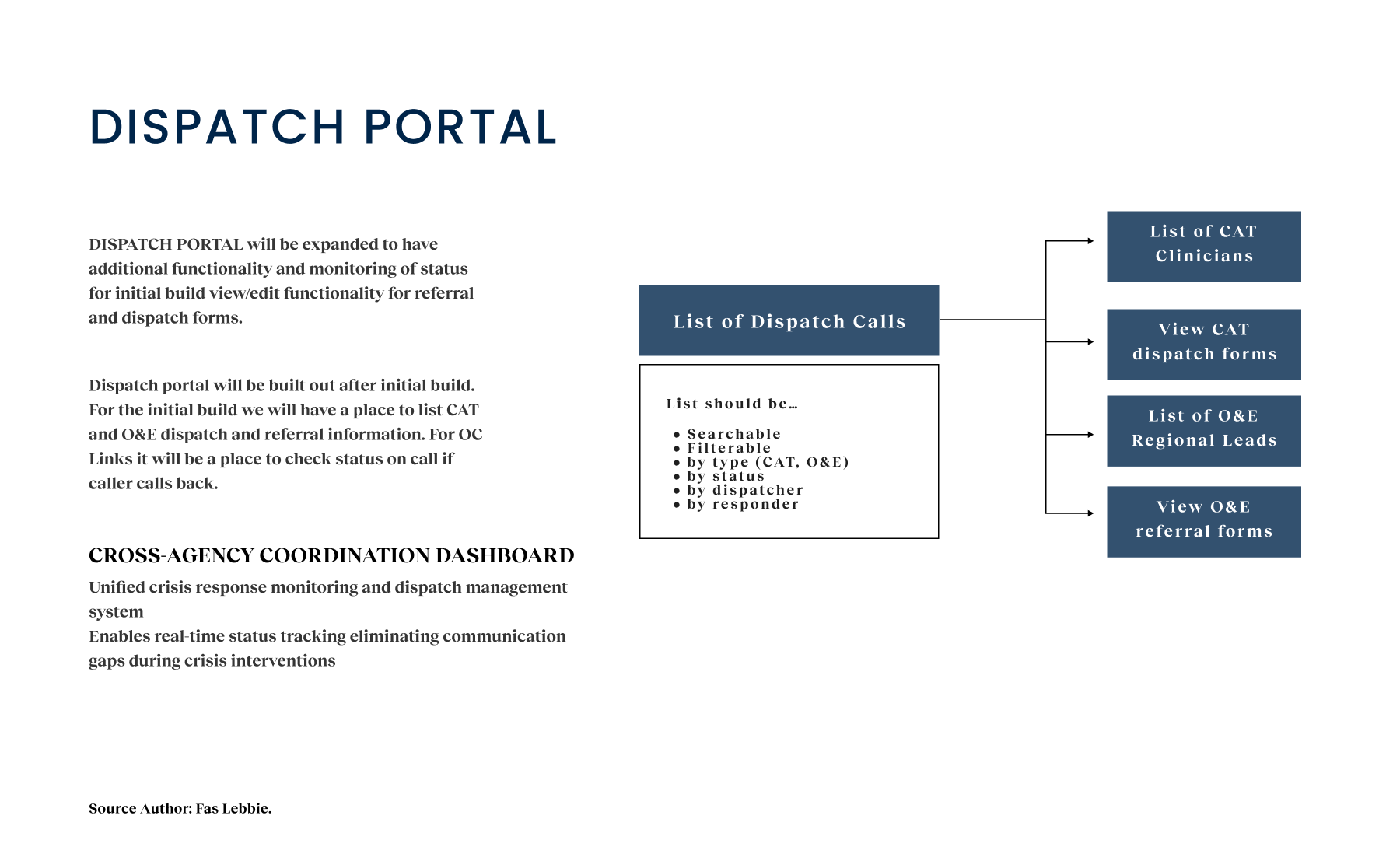
- Call tracking data revealed that 35% of cases involved multiple agencies (e.g., a transfer from NAMI to Crisis Assessment) but lacked a standardized method for information sharing. This was a critical failure point where context was often lost(handoff black hole). Design Implication: We needed a shared digital record that traveled with the user, regardless of which agency was handling the current step.
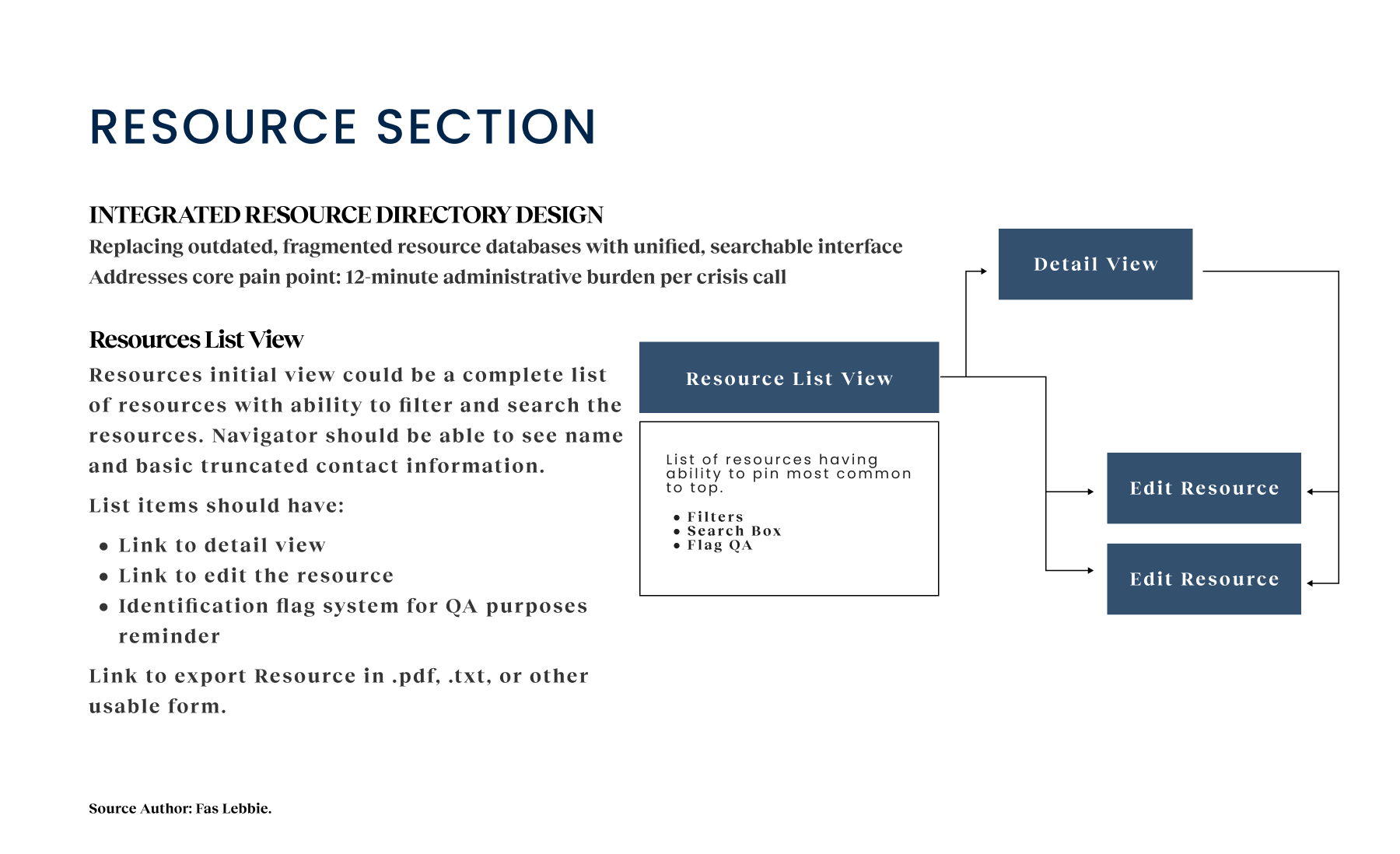
- The resource, the lifeblood of a referral service, was outdated and hard to navigate. Responders didn’t trust the data, leading to inconsistent service delivery. We needed an integrated resource management system that was easy to update and search in real-time.
- We found significant variance in the staff’s technological proficiency. A complex, “power-user” interface would fail. The UI had to be intuitive and accessible, with clear visual hierarchies to support decision-making under stress.
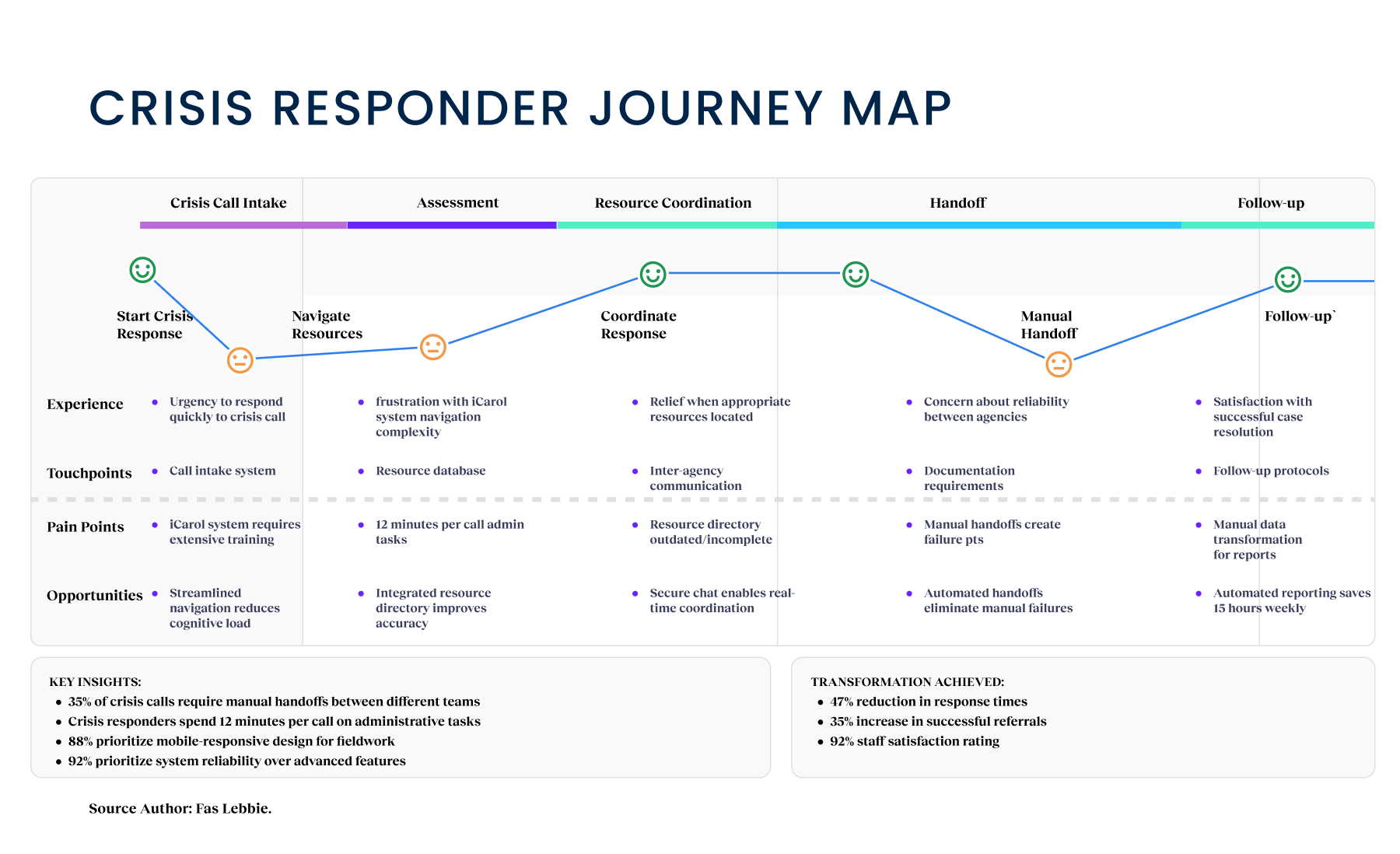
Goal: Reducing Cognitive Load. Responders were drowning in an “administrative tax,” spending 12 minutes per call on manual data entry and navigation rather than on direct care. We aimed to slash administrative steps by tracking “Time Spent on Administration,” freeing up cognitive capacity for clinical empathy and reducing the 15 hours of wasted time per responder per week.
Goal: Accelerating Care Velocity. A fragmented legacy system (iCarol) created dangerous delays during handoffs, with no real-time data flow between the three critical agencies. We focused on “Response Time Reduction,” hypothesizing that a unified platform would drastically cut the friction between a resident’s cry for help and a clinical response.
Goal: Closing the Loop. In this case, the multi-agency cases lacked a standardized method for information sharing, often resulting in clients falling through “black holes” in the system. We want to prioritize “Referral Success Rates,” measuring how effectively the system matched a resident’s complex needs with a verified, available resource without data loss.
Strategically, we adopted a Phased Implementation approach. We knew that trying to launch everything at once for three different agencies was a recipe for disaster. We prioritized OC Links’ essential functionalities for Phase I to deliver quick value, then progressively rolled out features for the Crisis Assessment Team and NAMI in subsequent phases. This allowed us to test reliability with a smaller cohort before scaling to the entire $18M initiative. We focused our prototyping efforts on three critical components: streamlined call management, integrated resource referrals, and secure communication channels. We started with low-fidelity sketches to validate workflows with the county’s service flow diagrams, ensuring we weren’t breaking any regulatory requirements. From there, we moved on to higher-fidelity interactive prototypes. We conducted iterative usability testing with 18 participants across three distinct phases. This testing was humbling. 92% of participants prioritized system reliability above all else; flashy features didn’t matter if the system lagged, for example, in worst-case scenarios such as during a suicide prevention call. 76% highlighted streamlined information sharing between agencies. These findings shaped our development roadmap and feature prioritization, enabling the product team to address immediate tactical needs.
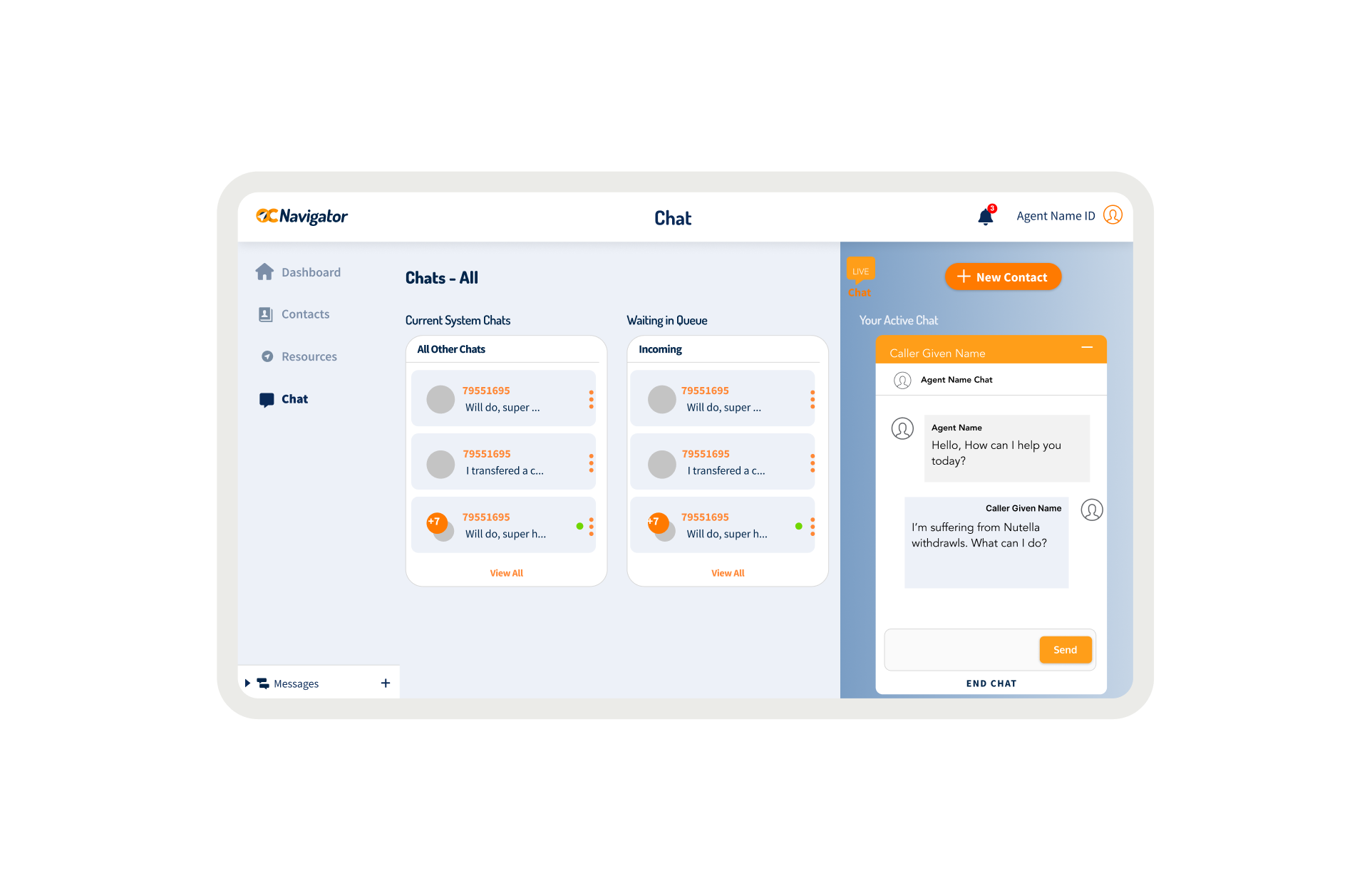
OC Links Platform Demo
Shows the streamlined crisis-response workflow enabling faster, safer coordination across Orange County’s behavioral-health system.
Design Interventions
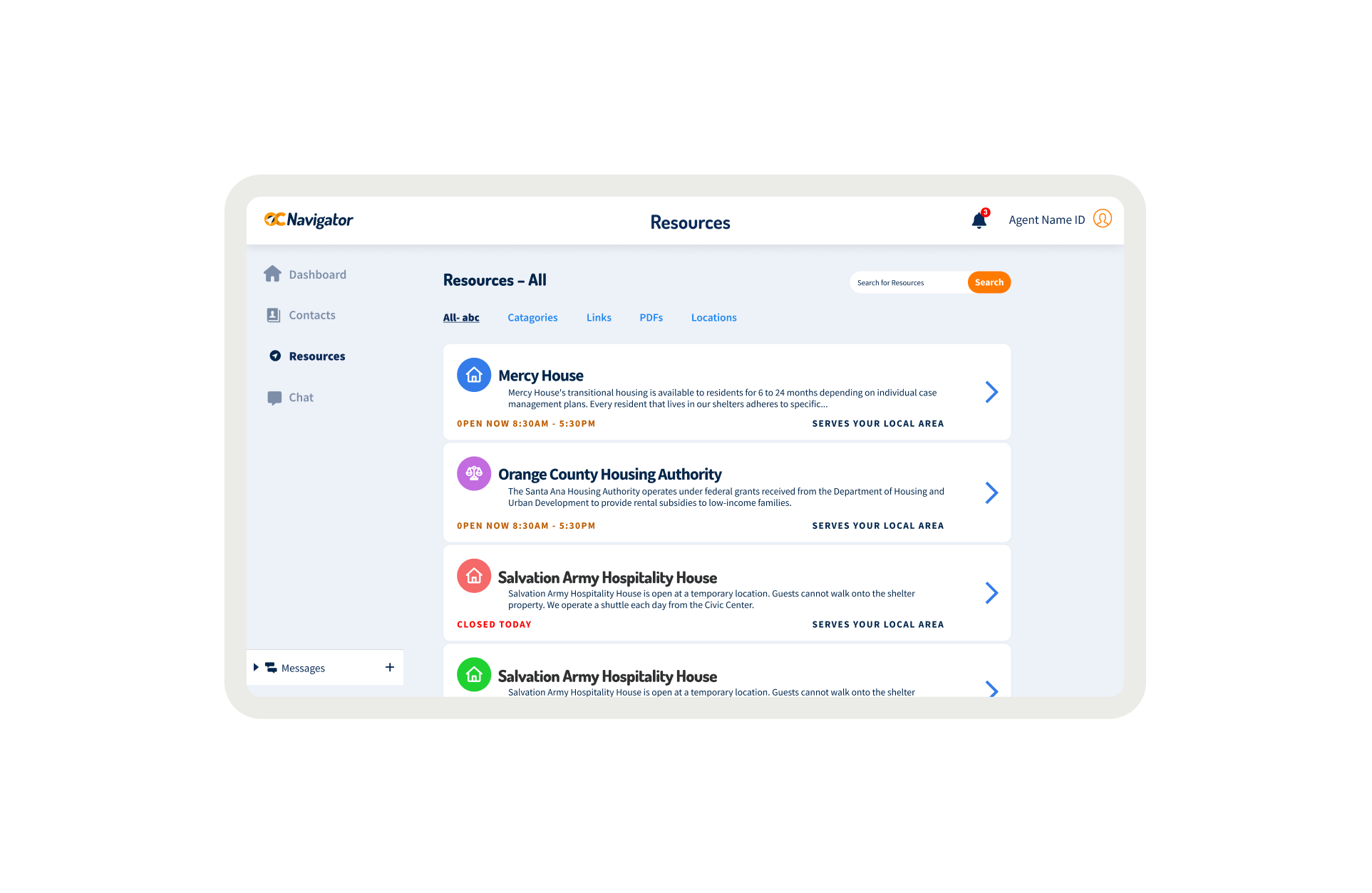
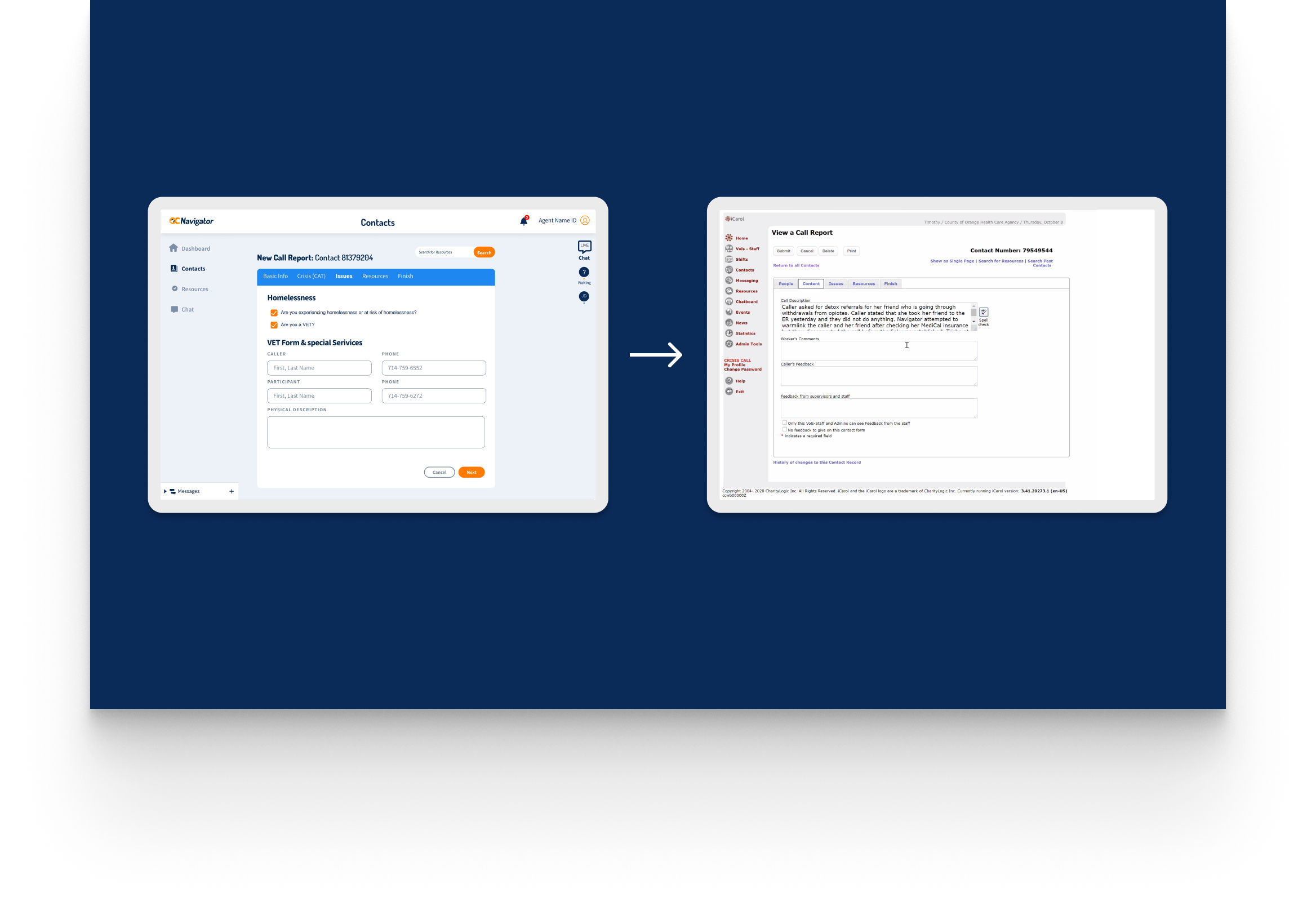
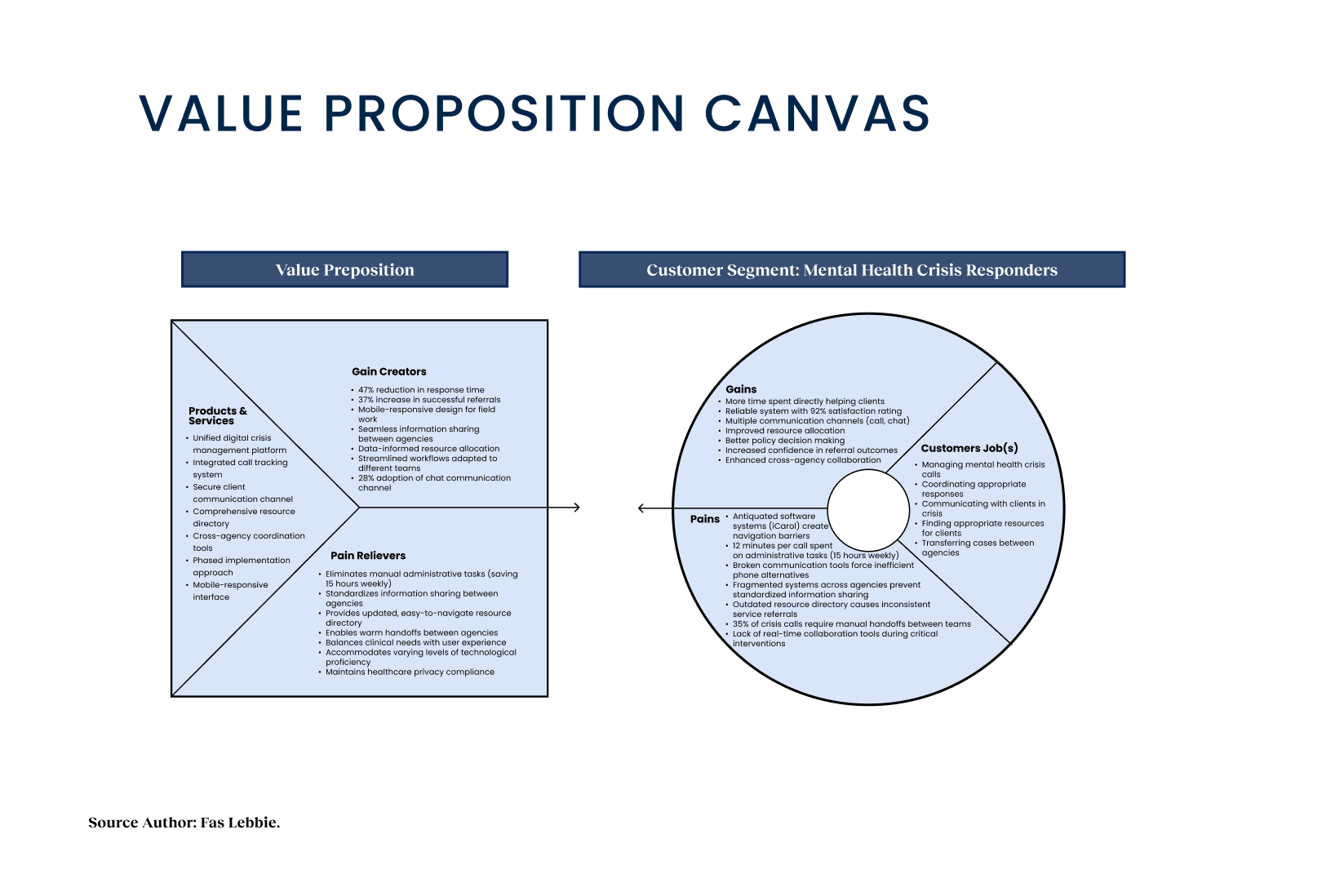
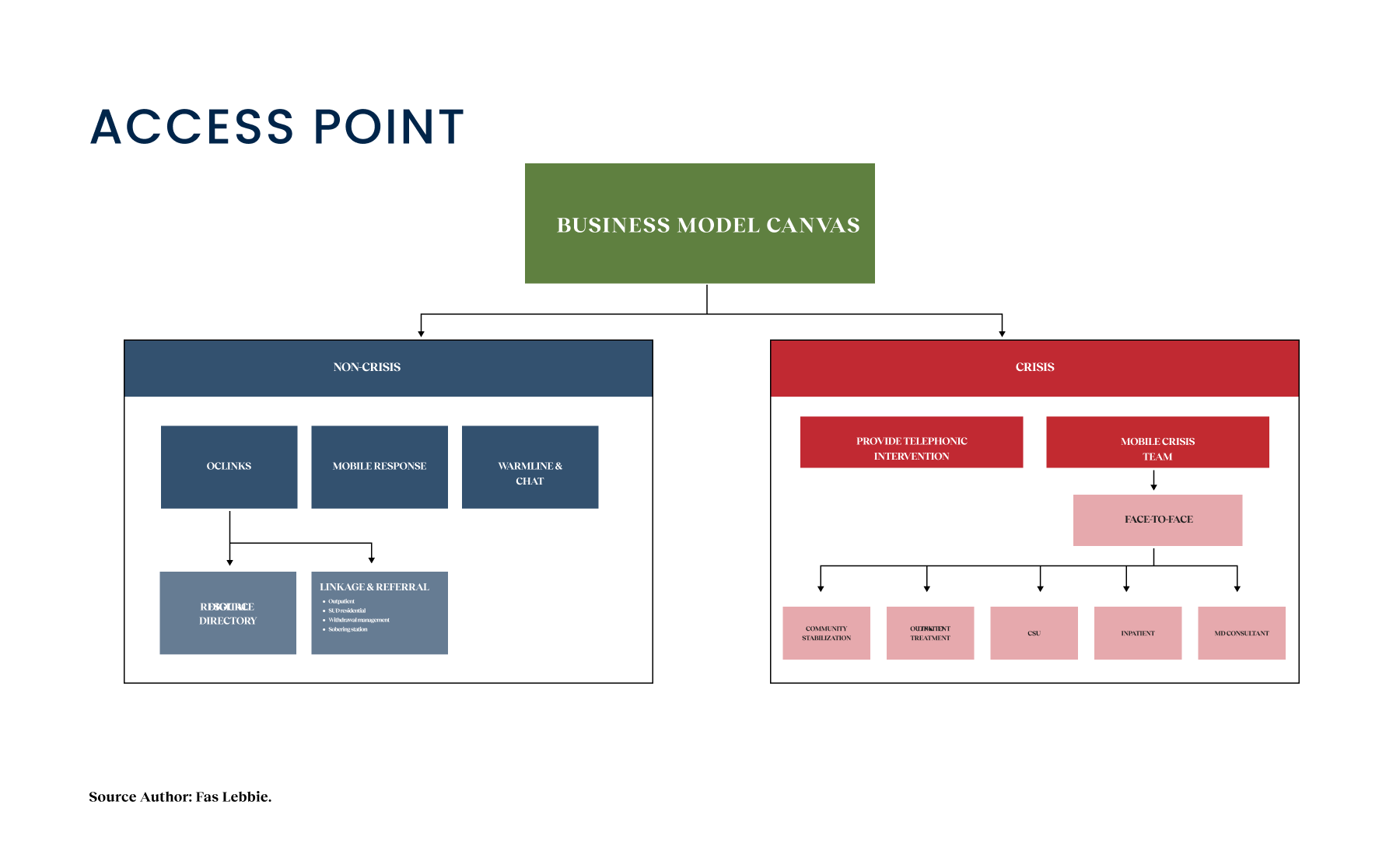
The core of our intervention was the creation of a unified digital platform for mental health crisis management. We replaced the isolated instances of iCarol with a single, integrated ecosystem that connects OC Links, the Crisis Assessment Team, and NAMI. This unified digital system streamlines workflows, reduces delays, and connects crisis responders with trusted resources instantly.
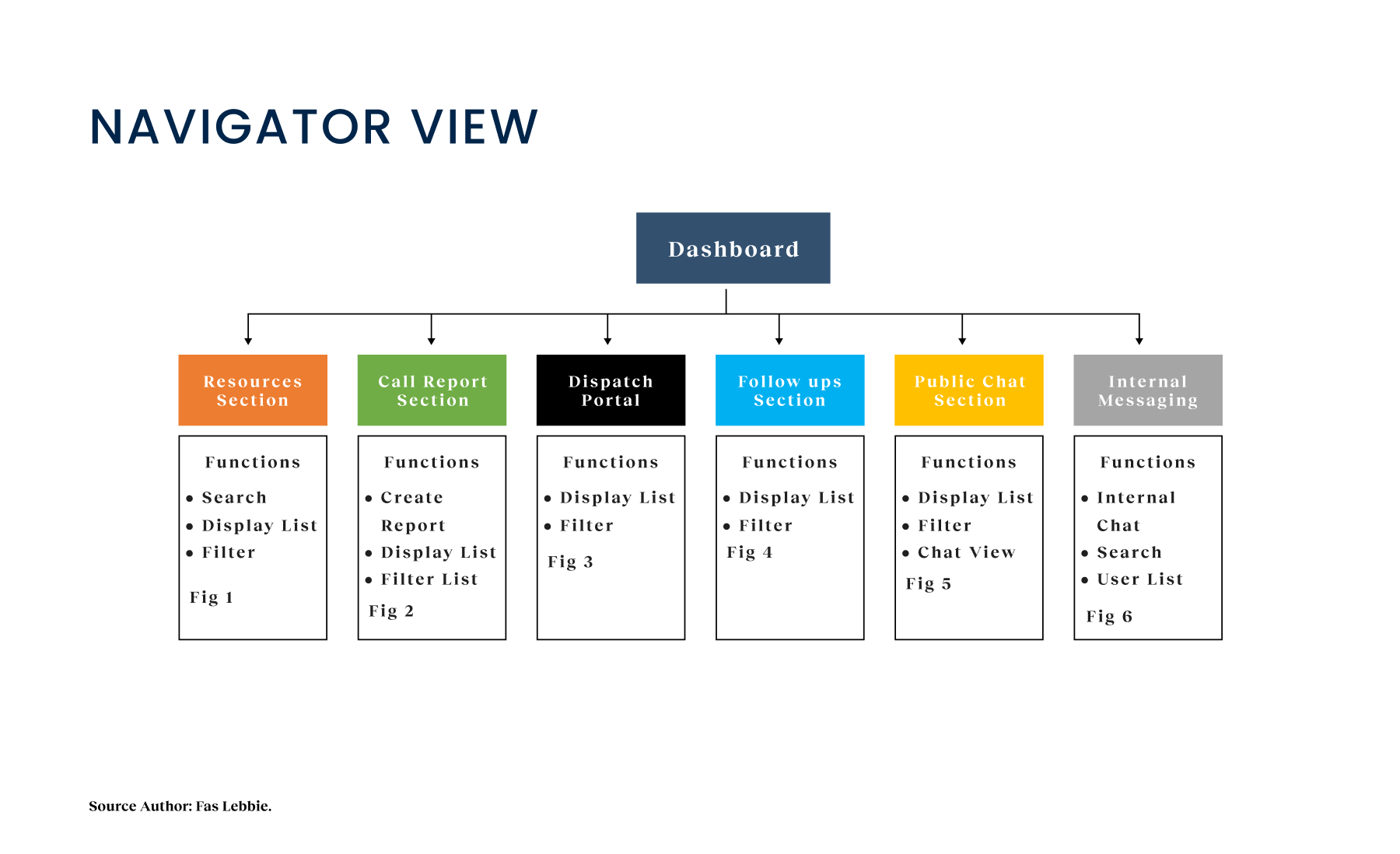
A complete redesign of the responder experience transformed how care is delivered. Our solution allows responders to manage calls, chat securely with clients, and access a verified resource directory without ever switching tabs. By integrating these workflows, we removed the friction of manual data transformation. We built a digital workflow that allows a case to be transferred between agencies while preserving context, eliminating the “black holes” where clients previously fell through the cracks. This system respects each agency’s varying privacy permissions while ensuring the person in crisis doesn’t have to repeat their story three times.

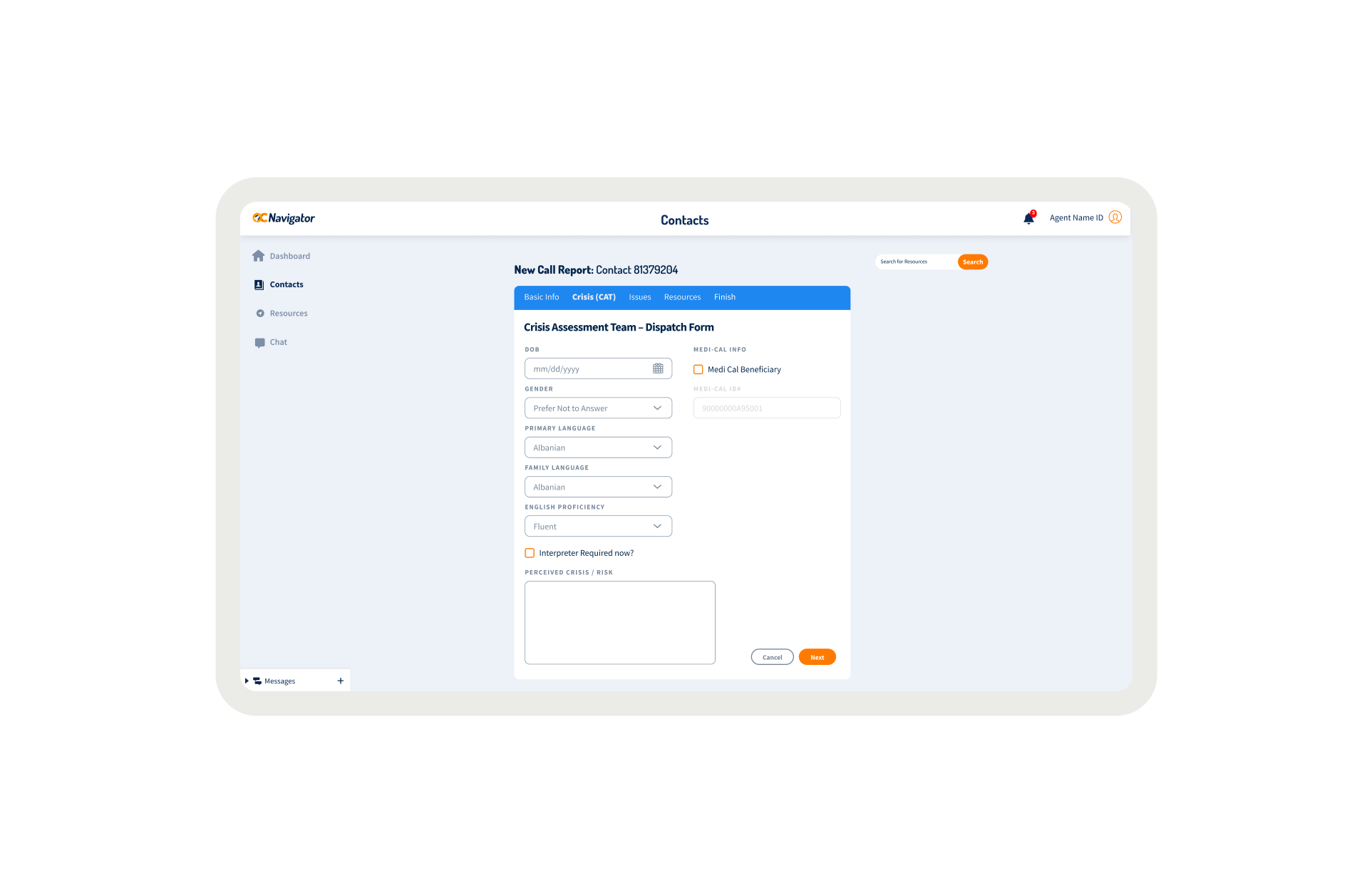
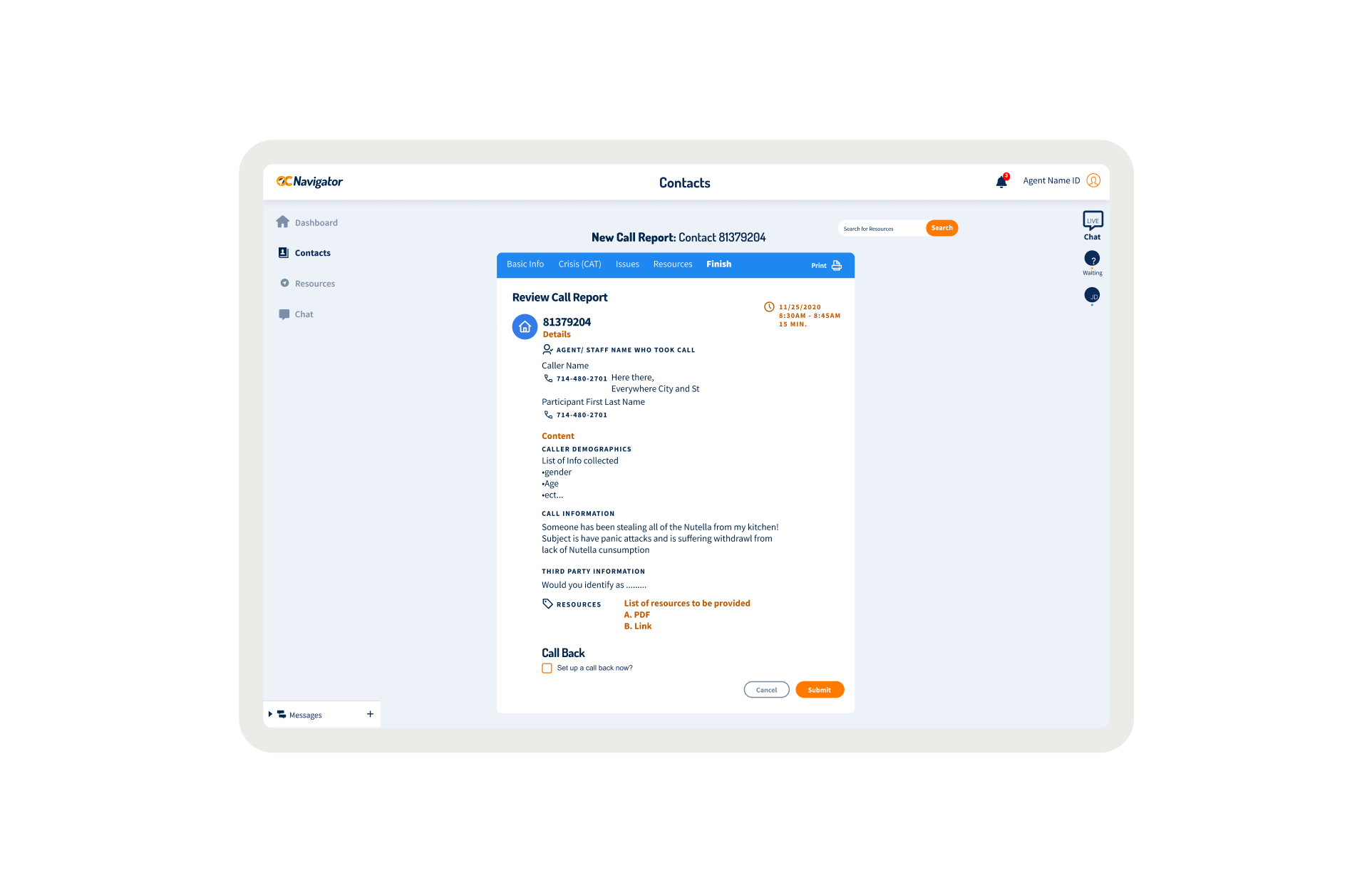
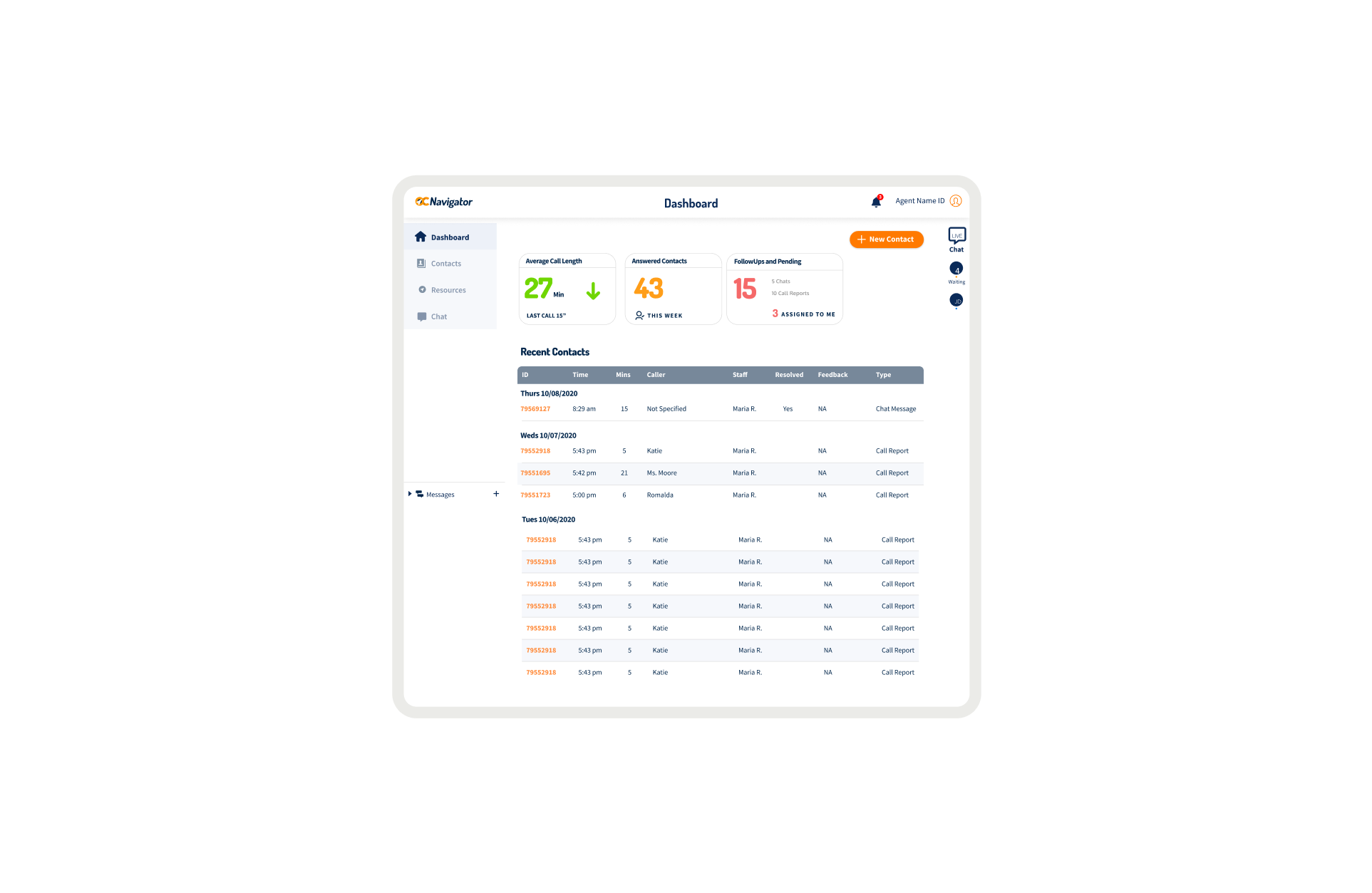
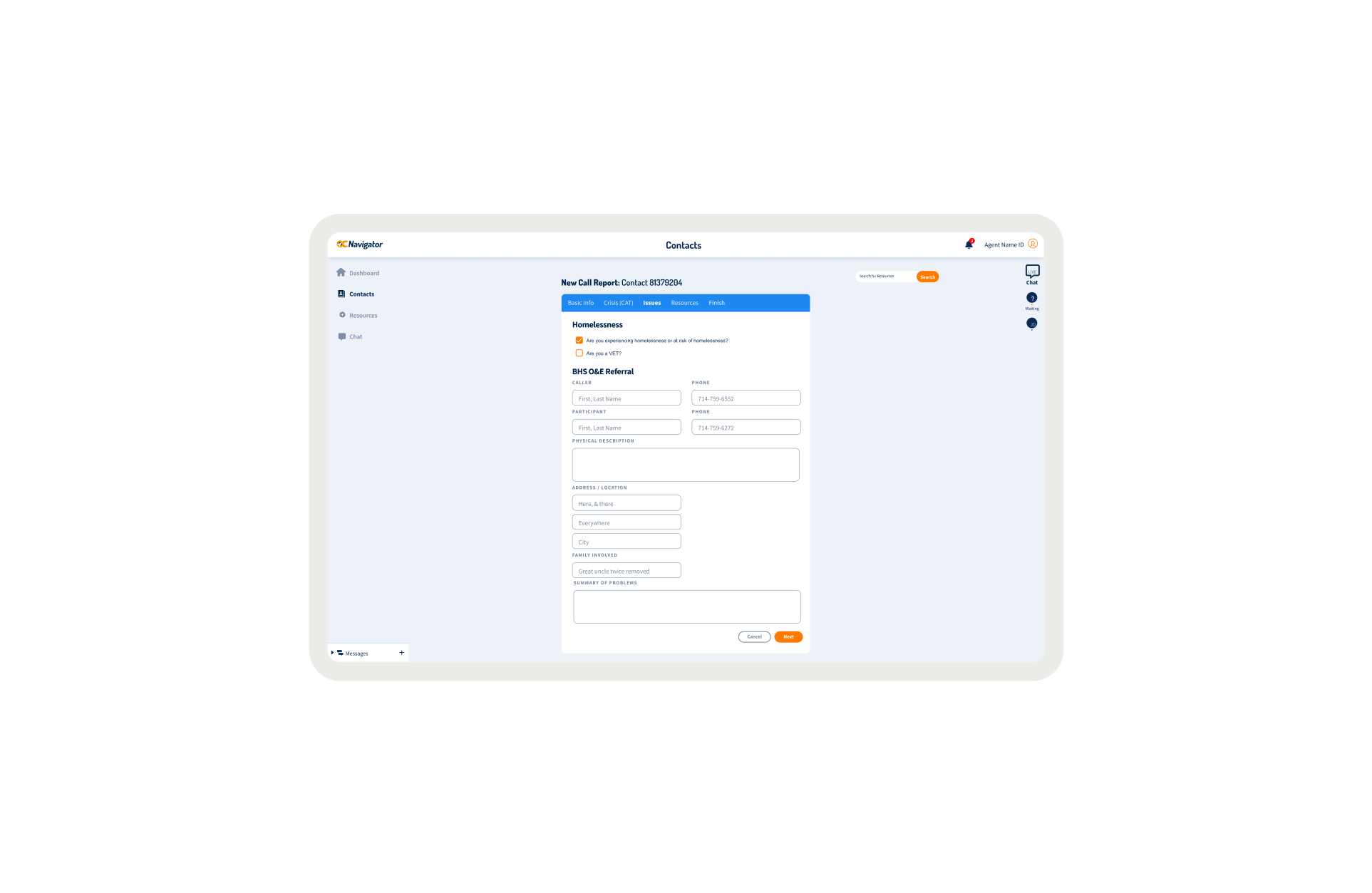
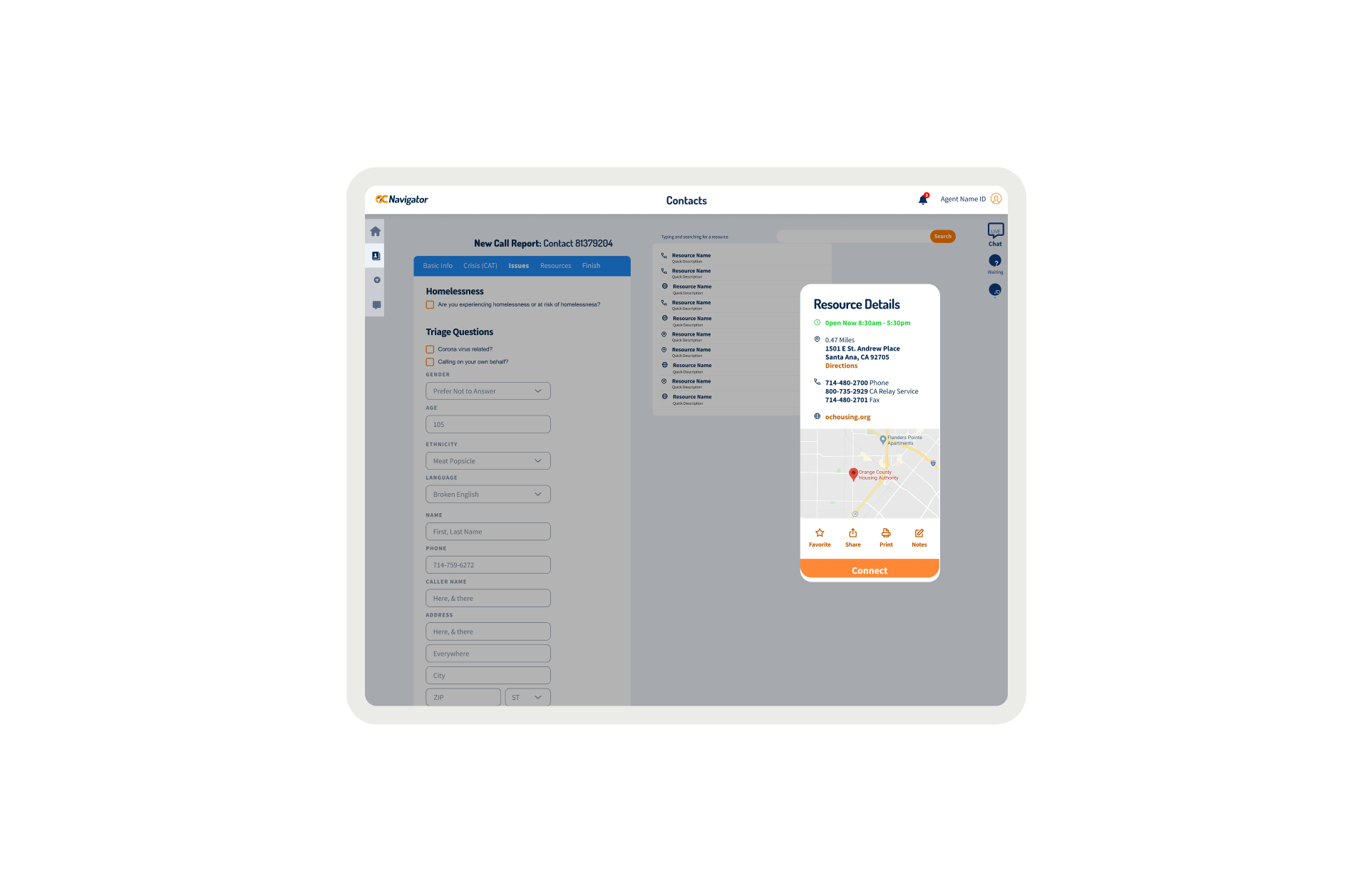
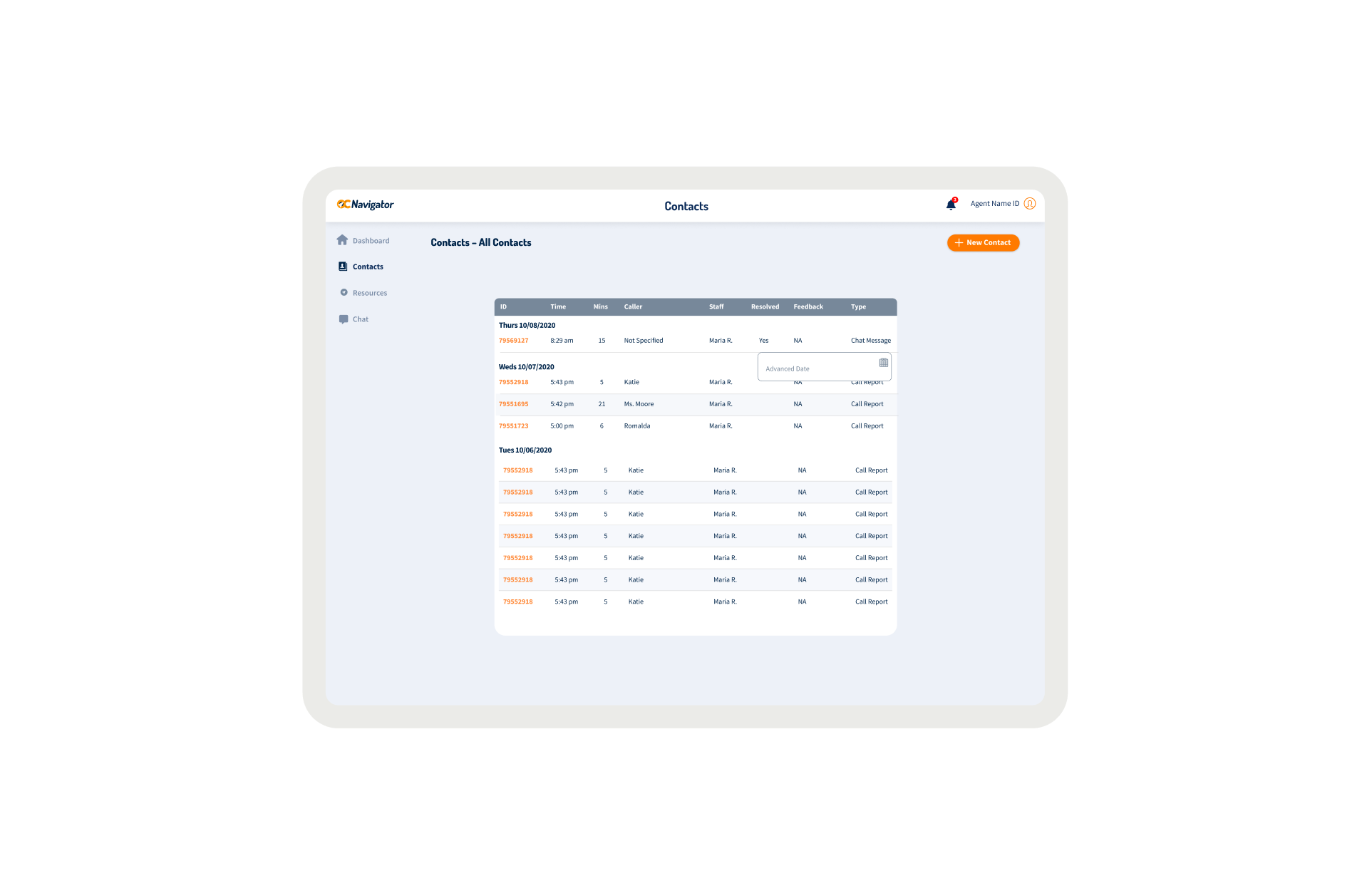
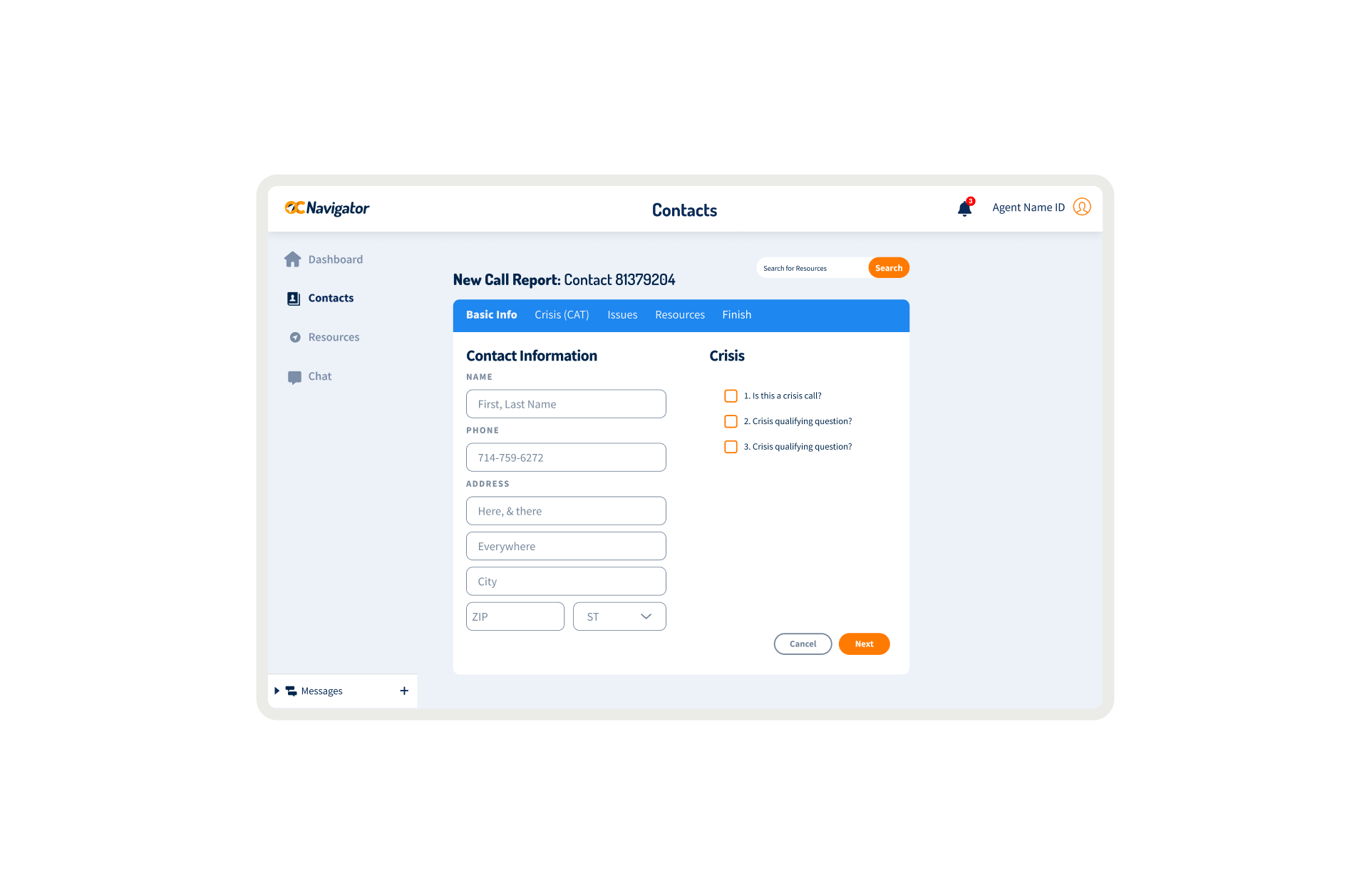
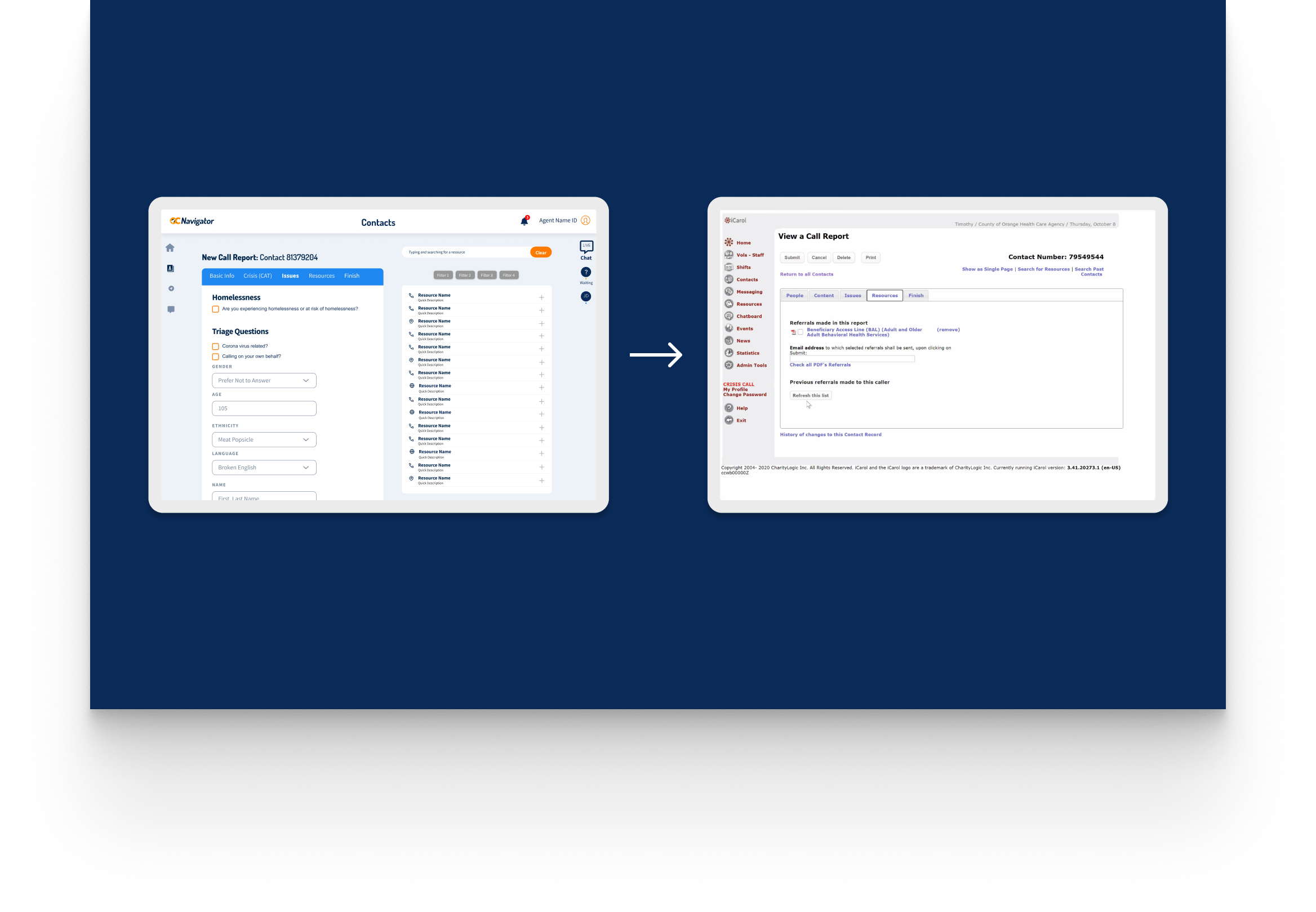
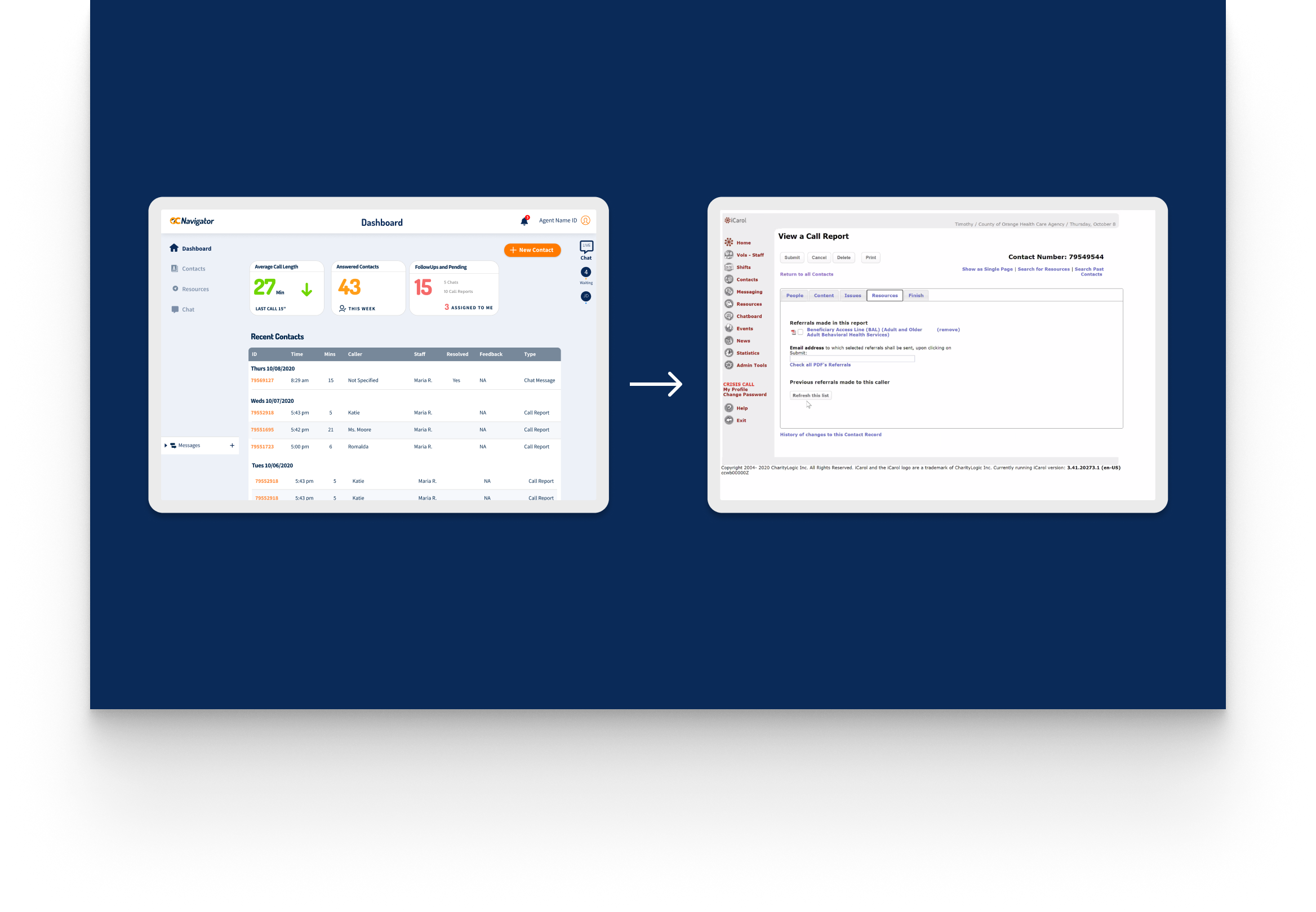
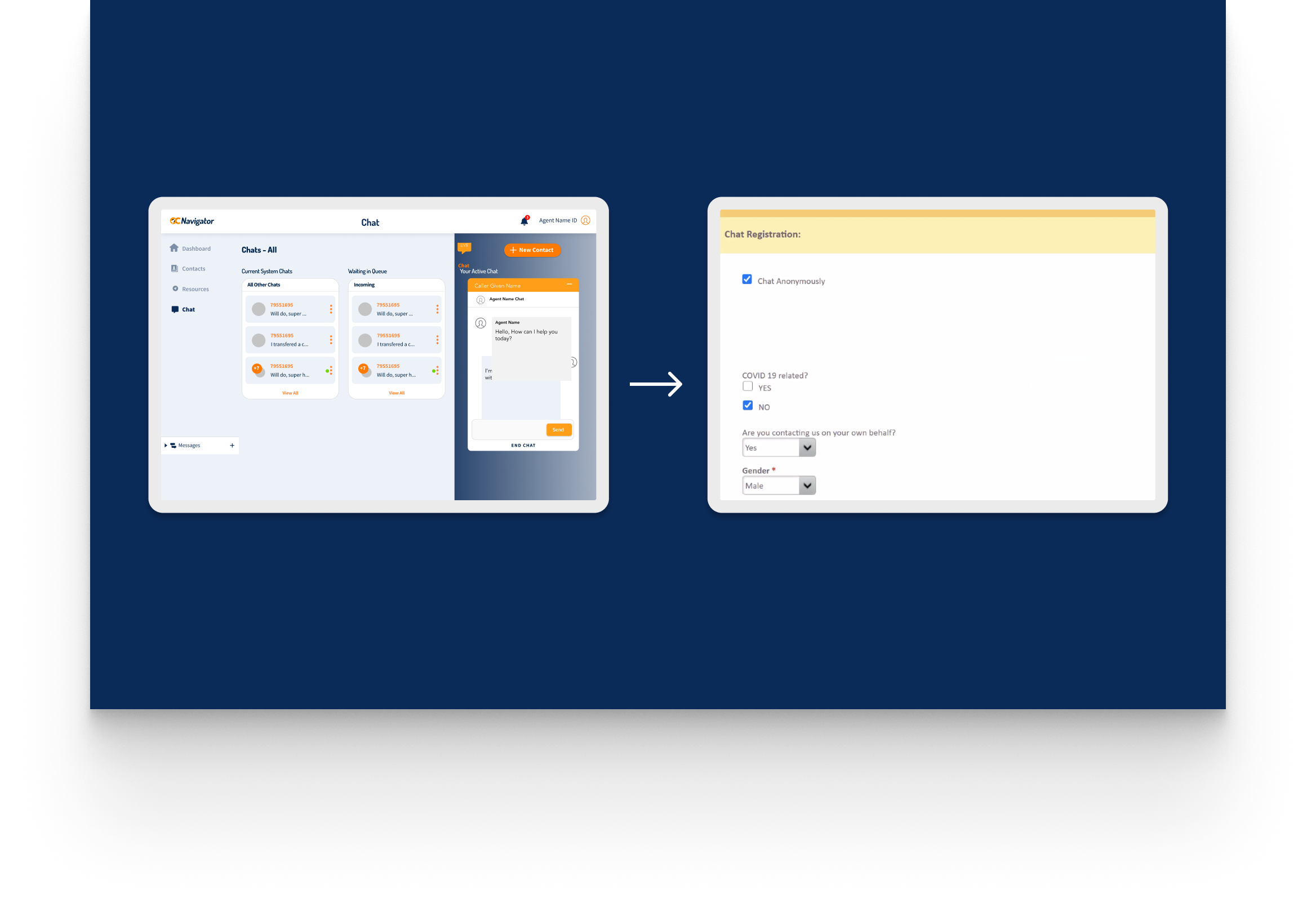
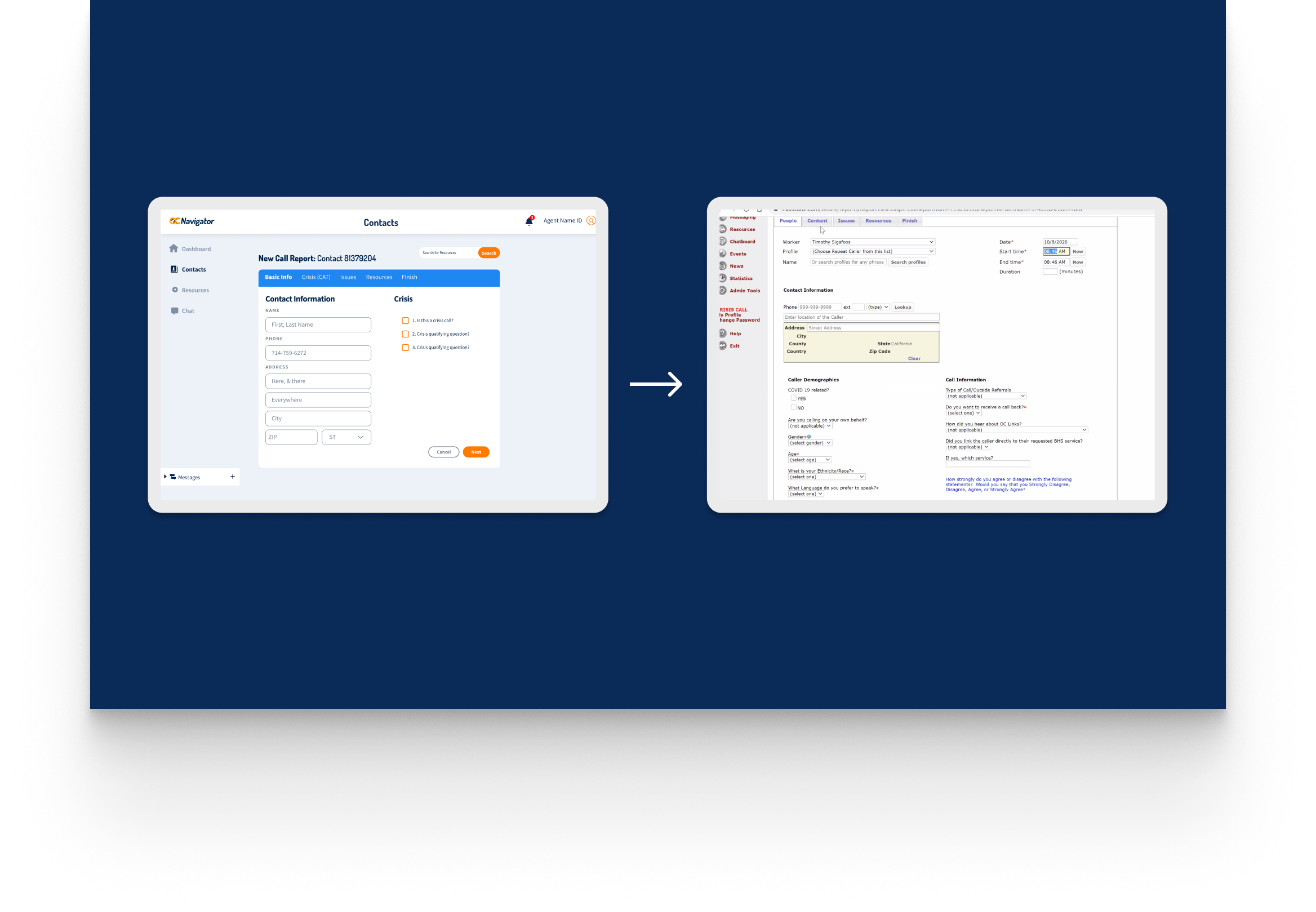
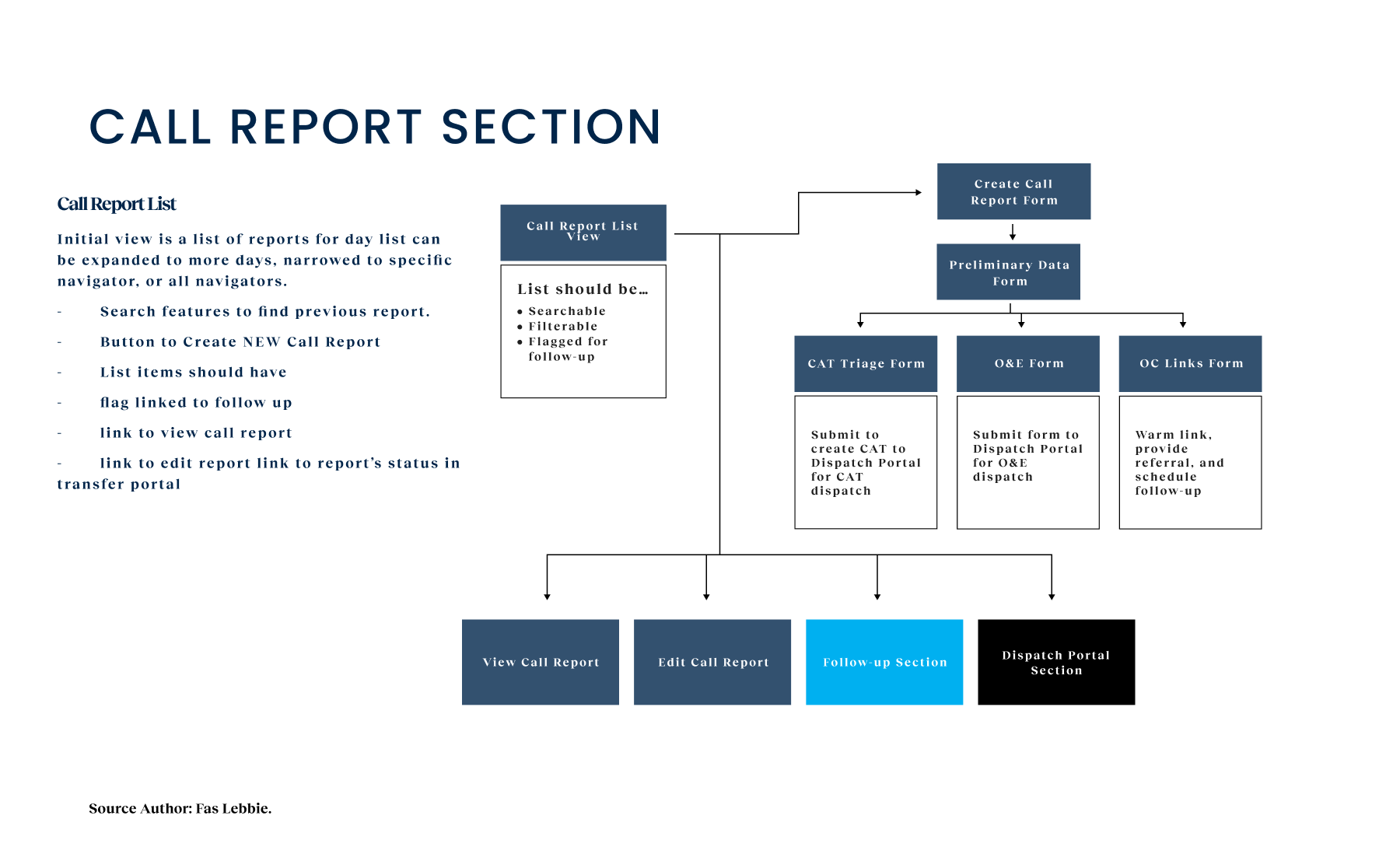
Crisis workers navigate contact intake, triage, referrals, and report documentation across desktop and mobile views. The workflow supports real-time coordination, allowing staff to log details, track follow-ups, and connect individuals to resources without losing context across different interaction points.

A unified digital system streamlines workflows, reduces delays, and connects crisis responders with trusted resources instantly.
Toolkit, Methods & Frameworks
This project was fundamentally a service design challenge disguised as a software project. We couldn’t just build a UI; we had to map the ecosystem. We used journey mapping, stakeholder activity mapping, value proposition canvas, and ecosystem mapping to understand the complex relationships among the county, non-profits, and hospital systems. We employed a theory-of-change framework to align these diverse partners around a shared vision. By visualizing the entire service blueprint from the moment a resident feels distress to the moment they are connected with long-term care, we identified the “informal workarounds” that were holding the old system together. This allowed us to formalize those pathways in the new digital tool, ensuring the software reflected the reality of the work rather than an idealized version.

Reduction of Crisis Response Times
Direct validation of our “Accelerating Care Velocity” goal; streamlined workflows eliminated the administrative bottlenecks that previously delayed critical interventions.
Staff Satisfaction Rating
Achieving our target to “Reduce Cognitive Load,” the shift from frustrated manual workarounds to reliable, unified tools transformed the daily responder experience.
Reflections & Impact
Looking back, the true impact of this work isn’t just in the efficiency metrics, though they are significant. It’s in the cohesion of the system. We transformed Orange County’s mental health response from a fragmented collection of “islands” into a unified safety net serving 650,000 residents. We operationalized this by shifting the definition of success from simple system uptime to “connection velocity.” By rigorously measuring friction points along the responder’s journey, we established a baseline showing that administrative drag was costing the $18M initiative millions in lost efficiency.
Operational improvements were immediate. The “administrative tax” that cost 15 hours per person per week was largely automated away, allowing staff to do what they do best: help people. We achieved a 47% reduction in average response times, effectively doubling the workforce’s capacity to handle crises without adding headcount. Simultaneously, successful referrals climbed by 35%, proving that when we automated the manual handoffs, patients actually received the care they needed. The 92% satisfaction rating tells me that we didn’t just build software the county wanted; we built the tools the staff actually needed to shift from frustration to reliability.
At an organizational level, the enhanced data-collection capabilities have created a “continuous feedback loop”. The county no longer has to guess where service gaps are; the data now informs resource allocation and policy decisions, establishing a new industry benchmark for how behavioral health networks can leverage design to address systemic inefficiencies.
Next Steps
- Launch a multilingual chat to introduce real-time translation features, broaden “Access Equity,” and capture the 28% of users who prefer text-based entry.
- Expand Integration by extending the platform to include additional county mental health services and community partners for a more connected crisis response ecosystem.
- Enhance field usability by developing mobile-responsive interfaces and multilingual chat to support Crisis Assessment Teams and Orange County’s diverse populations in real time.
- Implement Predictive Analytics: Utilize aggregated intake data to forecast resource demand, optimizing “Resource Allocation Efficiency” before surges occur.